Email: info@BSBortho.com
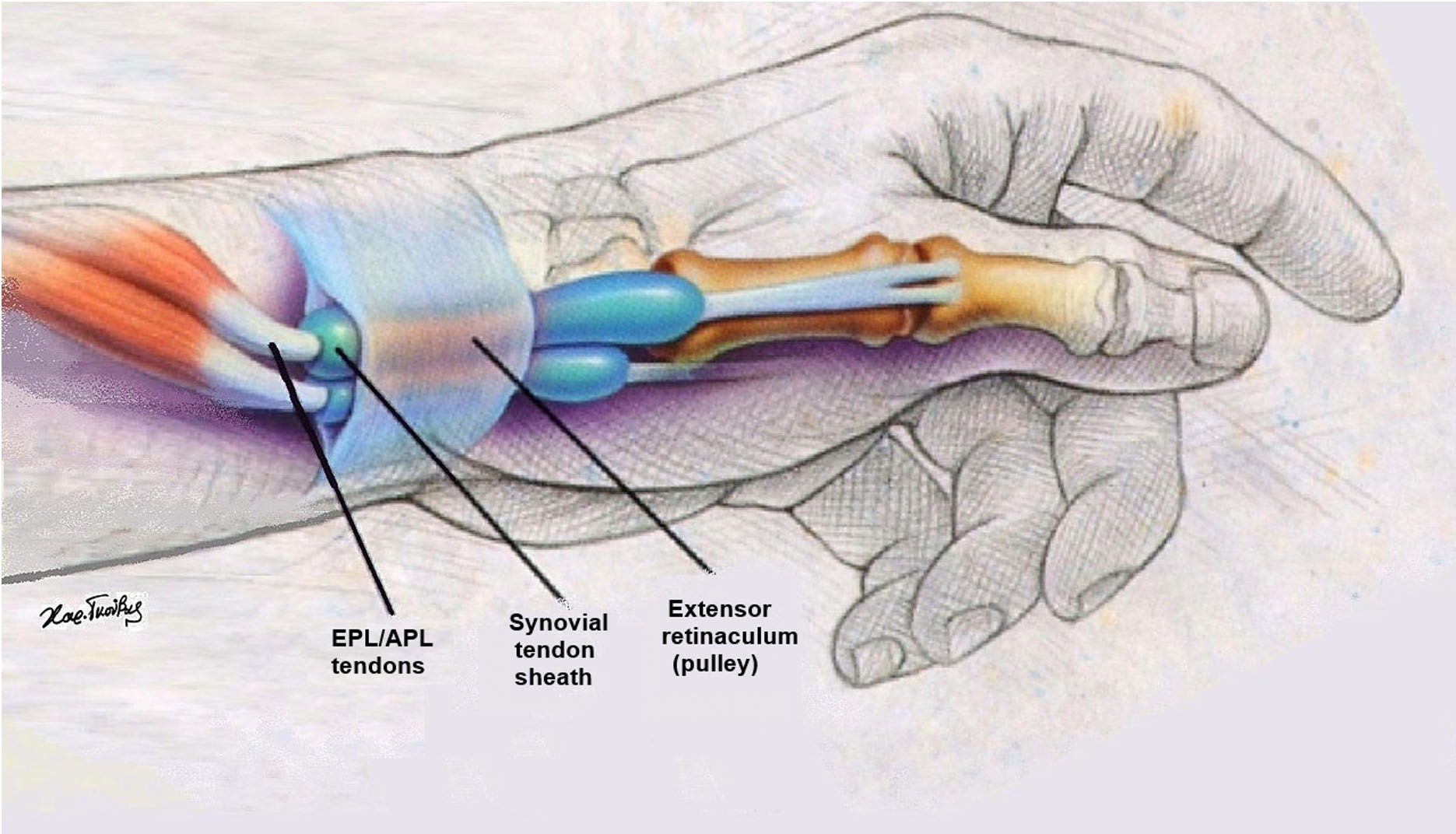
DeQuervain's Tenosynovitis is a condition that affects the tendons on the thumb side of the wrist. Inflammation between the tendon sheaths (the abductor pollicis longus (APL) and extensor pollicis brevis (EPB)) and the overlying pulley (or retinaculum) prevents the tendons from gliding smoothly in the first dorsal compartment during flexion and extension (Moore).
This condition is the most common tendinitis of the wrist in athletes (especially in golf, crew, baseball, and racquet sports). Unfortunately, it is particularly common among new mothers, hence its colloquial name "Mommy's Wrist" (Shehab et al.; Anderson et al.). The repetitive actions involved in caring for a newborn, such as lifting and holding the baby, carrying car seats, and positioning during breastfeeding, can contribute to the development of this condition.
The hallmark of DeQuervain's Tenosynovitis, include symptoms of pain, swelling, and difficulty moving the thumb and wrist. The pain can be worse with gripping or pinching, and as the condition progresses simple tasks become intolerable, including typing, texting, opening doors, and carrying a large Dunkin iced.
Typically DeQuervain's Tenosynovitis can be diagnosed using a clinical examination. If the pain can be reproduction when the tendons are passively stretched then this is considered a positive Finkelstein’s test, and can indicate DeQuervain's Tenosynovitis.
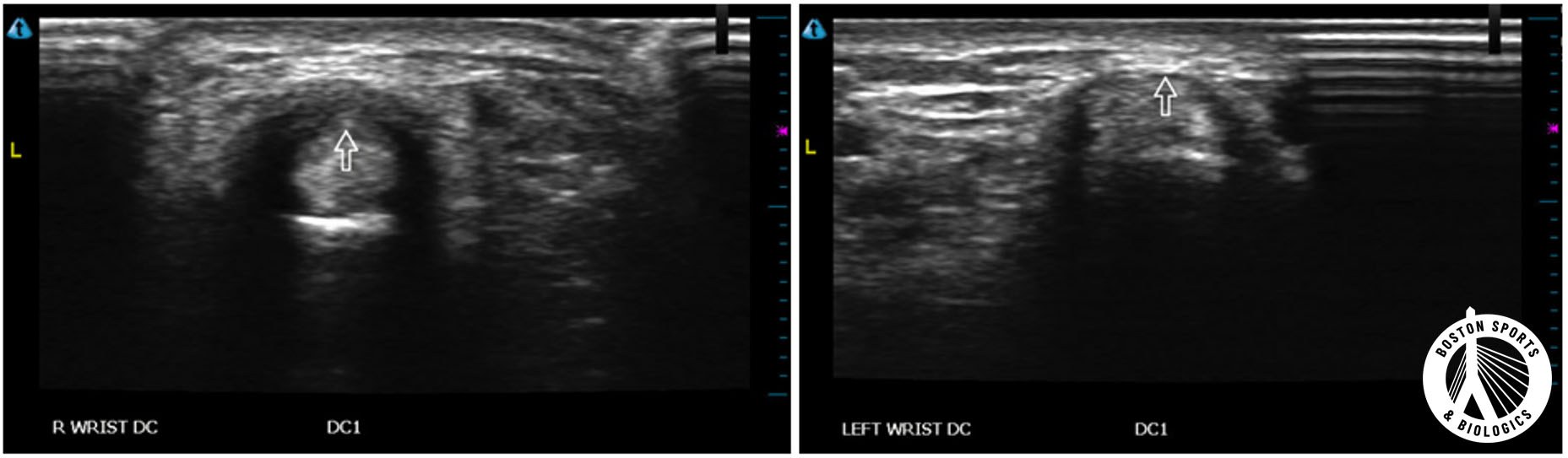
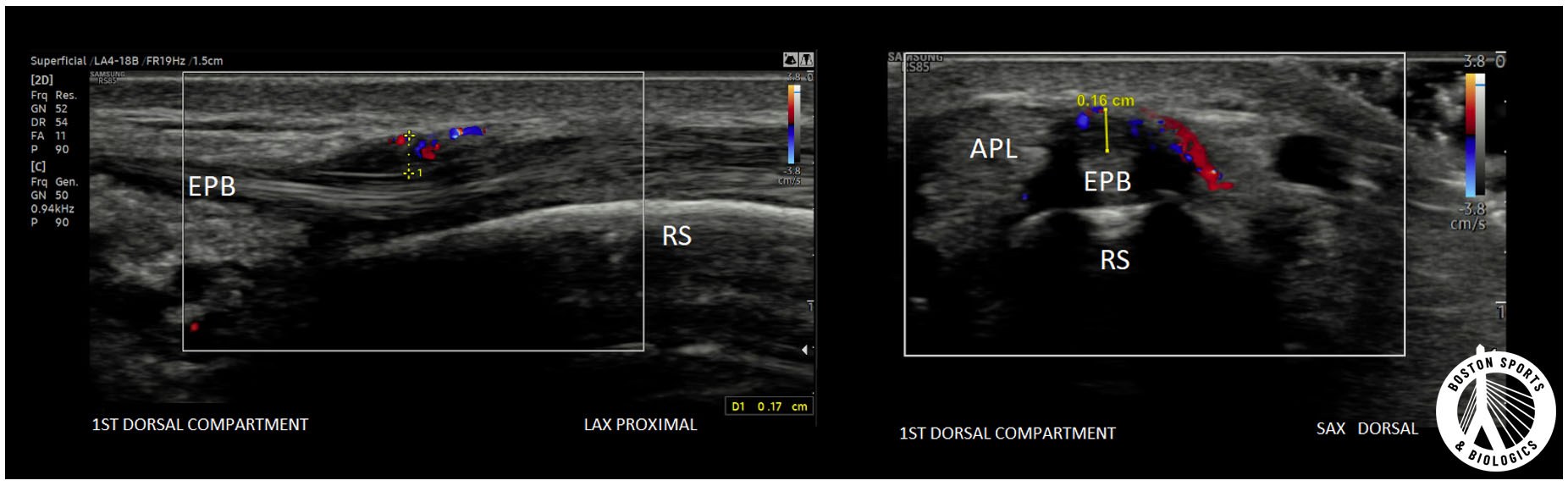
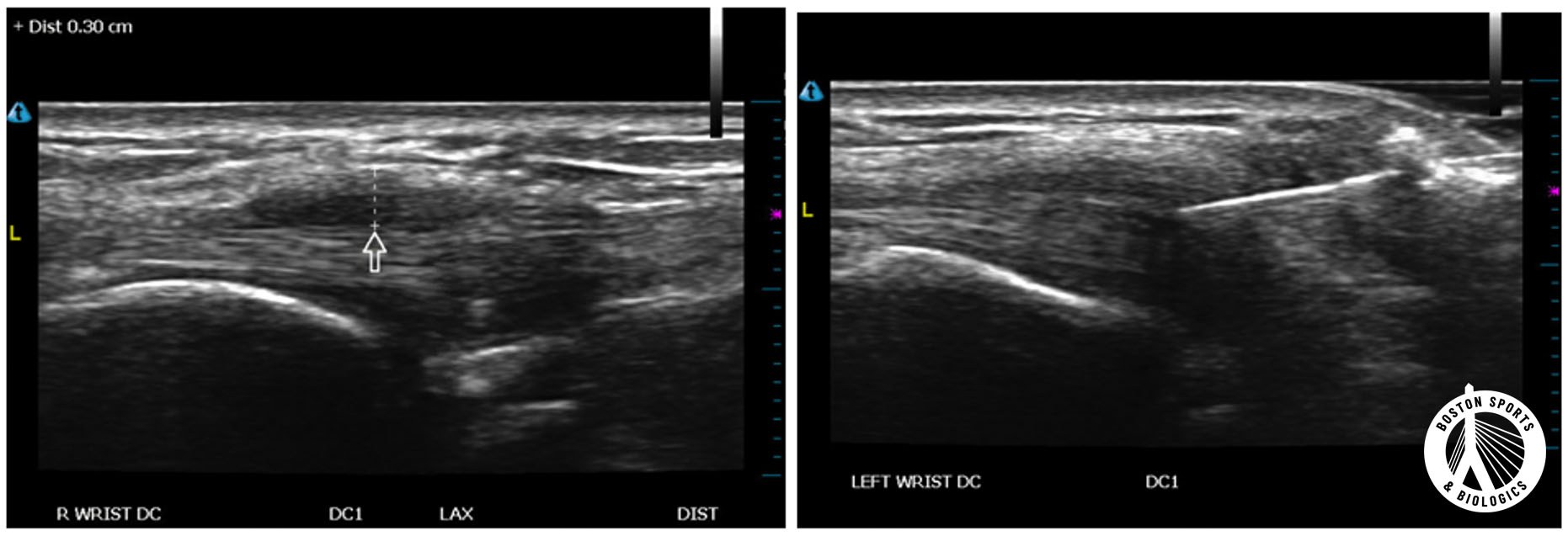
A diagnostic ultrasound at the initial visit can confirm the diagnosis by visualizing both a thickened extensor retinaculum (2-6x the normal thickness) and inflammation around the tendons and pulley (Lee et al.). Additionally, an ultrasound can assess for variations in the anatomy that may affect treatment (Volpe et al., Choi Et al.; Rousset et al.; Zaino et al.).
Initially, conservative treatments attempt to address inflammation and reduce overuse. include over the counter oral medications (Acetaminophen, Ibuprofen, Naproxen, etc), topical anti-inflammatories (diclofenac gel), thumb spica splints, and physical therapy, but evidence suggests that the most effective treatment is an ultrasound guided corticosteroid injection.
Corticosteroid injections
An ultrasound guided injection allows the medication to be precisely injected around into the tendon sheath and around the extensor retinaculum, without puncturing the tendon fibers themselves or the nearby superficial radial nerve.
Ultrasound-guieded steroid injections are effective in 83-97% of cases, and can be a first line treatment (Blood et al.; Ashraf et al.; Peter-Veluthamaningal et al.; Dande et al.; Jeyapalan et al.; McDermott et al.).
Surgery may be recommended if symptoms are severe or do not improve with non-operative management. The goal of surgery is to release the tendon sheath to make more room for the irritated tendons.
When corticosteroid injections don't resolve pain, an ultrasound-guided release of the first dorsal compartment release that can spare patients from traditional surgery surgery (Colberg et al.; Beidleman et al.). Ultrasound-guided release of trigger finger and carpal tunnel syndrome have results equal to or greater than surgery (Eberlin et al).
Similar to trigger finger releases, ultrasound-guided DeQuervain release is performed using imaging guidance to direct a Nokor needle to release the overlying extensor retinaculum, with only local anesthesia, minimal or no scar, and recovery in 2-3 days.
1. Anderson SE, Steinbach LS, De Monaco D, Bonel HM, Hurtienne Y, Voegelin E. "Baby wrist": MRI of an overuse syndrome in mothers. AJR Am J Roentgenol. 2004;182(3):719-724.
2. Ashraf MO, Devadoss VG. Systematic review and meta-analysis on steroid injection therapy for de Quervain’s tenosynovitis in adults. Eur J Orthop Surg Traumatol. 2014;24(2):149-57.
3. Beidleman MB, Colberg RE, Beason DP, Fleisig GS. A Retrospective Case Series Study on a Minimally Invasive Ultrasound-Guided First Dorsal Compartment Release Technique for Refractory De Quervain Tenosynovitis. American Journal of Physical Medicine & Rehabilitation. 2023 Mar 1;102(3):235-40.
4. Blood, T.D., N.T. Morrell, and A.P.C. Weiss, Tenosynovitis of the hand and wrist: A Critical Analysis Review. JBJS Reviews, 2016. 4(3): p. 8.
5. Choi SJ, Ahn JH, Lee YJ, et al. de Quervain disease: US identification of anatomic variations in the first extensor compartment with an emphasis on subcompartmentalization. Radiology. 2011;260(2):480-486.
6. Colberg RE, Henderson RG. Ultrasound-Guided First Dorsal Compartment Release for Refractory de Quervain Tenosynovitis: A Case Report. PM R. 2019;11(6):665-668.
7. Danda RS, Kamath J, Jayasheelan N, Kumar P. Role of Guided Ultrasound in the Treatment of De Quervain Tenosynovitis by Local Steroid Infiltration. J Hand Microsurg. 2016;8(1):34-37.
8. Eberlin KR, Amis BP, Berkbigler TP, Dy CJ, Fischer MD, Gluck JL, Kaplan FT, McDonald TJ, Miller LE, Palmer A, Perry PE. Multicenter randomized trial of carpal tunnel release with ultrasound guidance versus mini-open technique. Expert Review of Medical Devices. 2023.
9. Jeyapalan K, Choudhary S. Ultrasound-guided injection of triamcinolone and bupivacaine in the management of De Quervain's disease. Skeletal Radiol. 2009;38(11):1099-1103.
10. Lee, Kwang-Hyun, et al. "Ultrasonographic evaluation of the first extensor compartment of the wrist in de Quervain’s disease." Journal of Orthopaedic Science 19.1 (2014): 49-54.
11. McDermott JD, Ilyas AM, Nazarian LN, Leinberry CF. Ultrasound-guided injections for de Quervain's tenosynovitis. Clin Orthop Relat Res. 2012;470(7):1925-1931.
12. Moore JS. De Quervain's tenosynovitis. Stenosing tenosynovitis of the first dorsal compartment. J Occup Environ Med. 1997;39(10):990-1002.
13. Peters-Veluthamaningal C, Winters JC, Groenier KH, Meyboom-DeJong B. Randomised controlled trial of local corticosteroid injections for de Quervain's tenosynovitis in general practice. BMC Musculoskelet Disord. 2009;10:131.
14. Rousset P, Vuillemin-Bodaghi V, Laredo JD, Parlier-Cuau C. Anatomic variations in the first extensor compartment of the wrist: accuracy of US. Radiology. 2010;257(2):427-433.
15. Shehab R, Mirabelli MH. Evaluation and diagnosis of wrist pain: a case-based approach. Am Fam Physician. 2013;87(8):568-573.
16. Volpe, Alessandro, et al. "Ultrasound differentiation of two types of de Quervain's disease: the role of retinaculum." Annals of the rheumatic diseases 69.5 (2010): 938-939.
17. Zaino CJ, Mitgang JT, Rawat M, Patel MR. Anomalous muscles within the first dorsal extensor compartment of the wrist. Hand (N Y). 2014;9(4):551-553.
Learn how ultrasound-guided percutaneous fasciotomy may revolutionize treatment for chronic exertional compartment syndrome with faster recovery and smaller incisions.
Read MoreResearchers used artificial intelligence and natural language processing to identify Shoulder Injury Related to Vaccine Administration (SIRVA) cases from over 3.7 million vaccinations. Learn what the study found, how
Read More