Email: info@BSBortho.com
The median nerve travels through a narrow tunnel at the wrist and if compressed or irritated can cause carpal tunnel syndrome. Carpal tunnel syndrome is most common, and can cause symptoms of pain, numbness or tingling in the thumb, index finger, middle finger and ½ of the ring finger. Unless there is severe sensory loss or the motor function of the nerve is impacted then the initial treatment usually consists of a night splint and a carpal tunnel steroid injection.
Local cortisone injections are common practice, and have been shown to provide 1 month of relief when compared to a placebo injection. The dose of the steroid, type of steroid and site of injection do not seem to impact how effective cortisone injections are.
In most cases steroid injections can provide symptomatic relief, however, in one study of 281 injections in most cases symptom returned in 2 to 4 months. In this study 46% of the cases the steroid injection wore off work and patients underwent surgery (Green et al. 1984). In another study, surgery was eventually performed in 63% of hands after cortisone injections (Evers et al 2018a).
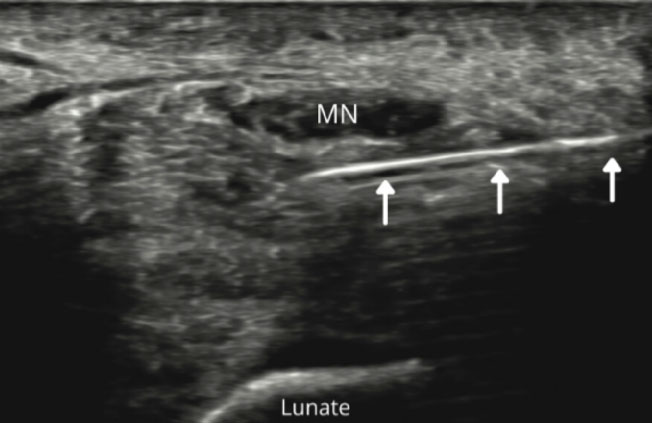
Nerve hydrodissection is a medical procedure that frees up scar tissue around a nerve. The nerve is localized using ultrasound and then using ultrasound guidance a needle guides medication around the nerve to free the nerve from any tissue that maybe compressing or entrapping the nerve.
Studies have shown that hydrodissection can be effective in treating carpal tunnel syndrome, and the volume of the injection can impact clinical outcomes. In one study, injections that used a higher volume had better outcomes, and and the type and dose of the steroid did not make a difference in the outcomes (Evers et al. 2018a).
In most of the studies looking at cortisone injections for carpal tunnel syndrome, the studies used a small volume of injectate, most commonly 1 to 3 mL (Evers et al. 2018a). Injections that use a smaller volume of fluid may have little or no contact with the nerve, and studies have shown that injections can have variable distribution around the nerve and carpal tunnel (Jariwala et al. 2013).
Fibrosis of the carpal tunnel connective tissue may play an important part in the pathophysiology of carpal tunnel syndrome (Ettema et al. 2004; Tat et al. 2015). This fibrotic tissue can compress the nerve and impact the blood flow to the nerve causing inflammation. Larger volume injections may have a greater effect hydrodissecting this fibrotic tissue (Evers et al. 2018a; Lin et al. 2020). These higher volume injections may reduce adhesions trapping the nerve.
Multiple randomized controlled studies have shown positive results from hydrodissection of the median nerve with improvements in pain and function (Tat et al. 2015; Salman Roghani et al. 2018; Wu et al. 2019). In one of these studies, the results were similar when injecting steroids or only numbing and saline. This suggests that the volume play an important a role in improving symptoms (Salman Roghani et al. 2018).
In another study, hands injected with a higher volume of fluid were more likely to have good long-term relief and avoid further treatment or surgery (Evers et al. 2018a). Another study showed improved nerve gliding in the carpal tunnel after hydrodissection (Evers et al. 2018b).
Many different injection techniques have been described. Traditionally carpal tunnel injections have been performed with the guidance of local anatomic landmarks, or a “blind” injection without any way of visualizing the nerve. Physician preforming “blind” injections cannot ensure accurate needle placement. Improper placement of the injections can damage the nerve or decrease the efficacy of the treatment. In one study, the accuracy of landmark guided injection was only 76%. In this study, 1 in 4 injections was not around the nerve and in 9% of cases the needle pierced the median nerve (Green et al. 2020).
While isolated studies have shown similar outcomes with “blind” or ultrasound guided injections (Eslamian et al. 2017), in a recent large higher quality systematic review and meta-analysis ultrasound guided cortisone injections had better results compared to landmark injections (Yang et al. 2021).
In addition to patients with ultrasound-guided injection having a significant improvement in clinical, neurophysiological, and ultrasound parameters outcomes than blind injected patients, ultrasound injections were safter. Ultrasound-guided injection can verify the needle position within the carpal tunnel, ensure a successful injection and decrease the risk of median nerve injury.
In another study, patients that had a “blind” injection reported complications included tingling sensation in 40% of patients, while no complications were reported patients that underwent an ultrasound-guided injection of the carpal tunnel (Omar et al. 2018).
Cortisone injections can fail in severe cases of carpal tunnel syndrome, especially if there is severe numbness or motor weakness. Other factors can also cause an injection to fail or symptoms to recur, including:
Studies have shown that pre-operative carpal tunnel steroid injections can hurt the long-term results after surgical release (Vahi et al. 2014). Consider an ultrasound-guided hydrodissection instead of another cortisone injection.
Ultrasound-guided hydrodissection procedure is not a painful procedure. The procedure starts by identifying the nerve with ultrasound and the nerve is followed looking for areas of swelling and thickening.
Once the area of entrapment and/or scar tissue is identified, then the skin is sterilized and the needle advanced under constant ultrasound guidance to the affected nerve. The injectate is the placed around the nerve freeing the nerve up from surrounding scar tissue and adhesions compressing the nerve.
Hydrodissection of nerves is note a technique for beginners in ultrasound guided injections and requires advanced skills. Dr. Sussman has advanced training in ultrasound and is one of a few physicians in Massachusetts to be certified in diagnostic musculoskeletal ultrasound (RMSK) and to be trained in carpal tunnel release using ultrasound guidance and the Sonex-micro knife.
For more information on hydrodissection procedures for carpal tunnel syndrome contact us for a consultation with Dr. Sussman at:
References:
Eslamian F, Eftekharsadat B, Babaei-Ghazani A, Jahanjoo F, Zeinali M. A randomized prospective comparison of ultrasound-guided and landmark-guided steroid injections for carpal tunnel syndrome. J Clin Neurophysiol. 2017; 34: 107-113.
Ettema AM, Amadio PC, Zhao C, Wold LE, An KN. A histological and immunohistochemical study of the subsynovial connective tissue in idiopathic carpal tunnel syndrome. J Bone Joint Surg Am. 2004; 86: 1458-1466.
Evers S, Bryan AJ, Sanders TL, Gunderson T, Gelfman R, Amadio PC. Influence of Injection Volume on Rate of Subsequent Intervention in Carpal Tunnel Syndrome Over 1-Year Follow-Up. J Hand Surg Am. 2018 Jun;43(6):537-544.
Evers, S., Thoreson, A. R., Smith, J., Zhao, C., Geske, J. R., and Amadio, P. C. (2018). Ultrasound‐guided hydrodissection decreases gliding resistance of the median nerve within the carpal tunnel. Muscle Nerve 57 (1), 25–32.
Green DP. Diagnostic and therapeutic value of carpal tunnel injection. J Hand Surg Am. 1984;9A:850-854.
Green DP, MacKay BJ, Seiler SJ, Fry MT. Accuracy of Carpal Tunnel Injection: A Prospective Evaluation of 756 Patients. Hand (N Y). 2020 Jan;15(1):54-58.
Jariwala A, Zaliunaite R, Soames R, Wigderowitz C.A. Assessing the variability of injectate distribution following carpal tunnel injection—a cadaveric study. Hand Surg. 2013; 18: 313-316.
Lin MT, Liao CL, Hsiao MY, Hsueh HW, Chao CC, Wu CH. Volume Matters in Ultrasound-Guided Perineural Dextrose Injection for Carpal Tunnel Syndrome: A Randomized, Double-Blinded, Three-Arm Trial. Front Pharmacol. 2020 Dec 17;11:625830.
Omar G, Ali F, Ragaee A, Darwiesh A. Ultrasound-guided injection of carpal tunnel syndrome: A comparative study to blind injection. The Egyptian Rheumatologist. 2018; 40(2):131-135
Salman Roghani R, Holisaz MT, Tarkashvand M, Delbari A, Gohari F, Boon AJ, Lokk J. Different doses of steroid injection in elderly patients with carpal tunnel syndrome: a triple-blind, randomized, controlled trial. Clin Interv Aging. 2018 Jan 18;13:117-124.
Tat J, Wilson KE, Keir PJ. Pathological changes in the subsynovial connective tissue increase with self-reported carpal tunnel syndrome symptoms. Clin Biomech (Bristol, Avon). 2015; 30: 360-365.
Vahi PS, Kals M, Kõiv L, Braschinsky M. Preoperative corticosteroid injections are associated with worse long-term outcome of surgical carpal tunnel release. Acta Orthop. 2014 Feb;85(1):102-6.
Wu YT, Chen SR, Li TY, Ho TY, Shen YP, Tsai CK, Chen LC. Nerve hydrodissection for carpal tunnel syndrome: A prospective, randomized, double-blind, controlled trial. Muscle Nerve. 2019 Feb;59(2):174-180.
Yang, FA., Shih, YC., Hong, JP. et al. Ultrasound-guided corticosteroid injection for patients with carpal tunnel syndrome: a systematic review and meta-analysis of randomized controlled trials. Sci Rep. 2021;11:10417.
Learn how ultrasound-guided percutaneous fasciotomy may revolutionize treatment for chronic exertional compartment syndrome with faster recovery and smaller incisions.
Read MoreResearchers used artificial intelligence and natural language processing to identify Shoulder Injury Related to Vaccine Administration (SIRVA) cases from over 3.7 million vaccinations. Learn what the study found, how
Read More