Email: info@BSBortho.com

I recently had lunch with one of my physician friends who had a PRP injection into his rotator cuff and biceps tendon. He was upset because he was a few months out from the injection, and had not noticed a big difference in his pain.
There is a growing recognition that rotator cuff tears and
biceps tendon pathology are closely related. One challenge we see in our clinic is that partial
biceps tendon tears are often missed. Some of our patients will even have rotator
cuff surgery that only targets the rotator
cuff and misses the biceps tendon leaving them with continued pain over the front of the
shoulder.
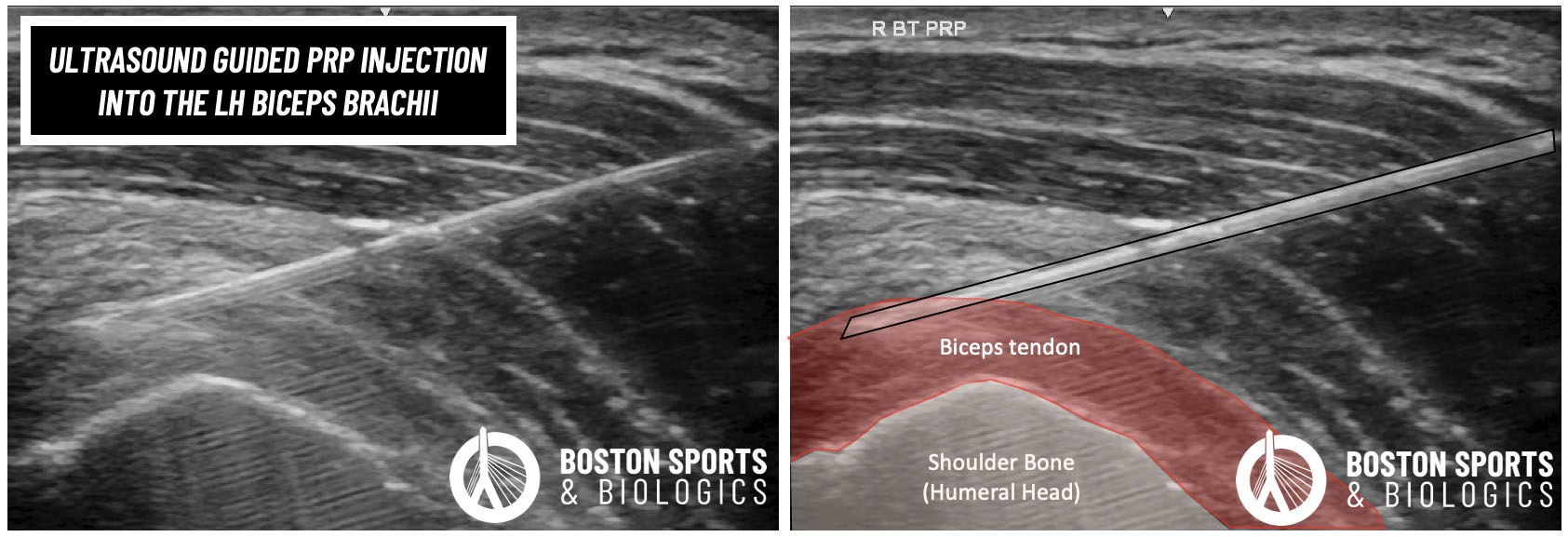
In my friends case they injected PRP into the biceps tendon, but equally important is making sure the PRP reaches the source of pain. In most injection text books they teach to inject the biceps tendon in the front of the shoulder. The problem is that most of these books are teaching how to inject cortisone around a tendon, but when injecting PRP it has to be directed into the frayed and torn tendon. In the case of the biceps tendon, this is higher up than where these text books teach us to injection.... and this was the problem with my friends case.
Learn more about rotator cuff tears and biceps tendon pain below and the importance of placing these injections correctly.
The long head of the biceps brachii tendon arises within the shoulder joint capsule, and exits the joint deep to the supraspinatus and subscapularis rotator cuff tendons in the rotator interval. This means that the long head of the biceps tendon sits just deep to the rotator cuff tendon, and can also be injured along with the rotator cuff tear.
The clinical presentation of long head biceps tendon and rotator cuff pathology are similar. SLAP lesions a involve a tear of the long head of the biceps tendon at its anchor within the shoulder joint and can also have overlapping symptoms.
Clinical exam findings can sometimes distinguish between these two tendinopathies, but often imaging with musculoskeletal ultrasound or MRI is needed to confirm the diagnosis. Differential injections can also help confirm the location of pain.
Biceps brachii tendon pain is likely under recognized, and commonly co-occurs with rotator cuff tears. In patients with a complete rotator cuff tears, in one study over 2/3 of the patients also had a long head of biceps tendon abnormality (Murthi et al 2000). In another study, over 90% of patients with long head of biceps tendon pathology had simultaneous rotator cuff tears (Chen et al 2005).
In orthopedics, these injuries are often managed conservatively with NSAIDs, activity modification, physical therapy and cortisone injections. However, pain from the biceps brachii tendon is rarely due to inflammation. In fact, there is no evidence that the root cause of biceps tendon pain is from acute inflammation of the tendon. Histologic studies looking at the tendon architecture under a microscope showed no evidence of acute inflammation, and tendon changes are consistent with chronic degenerative process (Streit et al 2015).
Platelet rich plasma (PRP) injections has been well studies in the shoulder for the rotator cuff (learn more here). One limitation to these studies is that in many cases the biceps brachii tendon was not treated with the rotator cuff. As discussed above these lesions often co-occur, and PRP has been shown to be helpful for proximal biceps tendinitis (Moon et al 2011).
In surgery, when lesions of the biceps brachii tendon are detected during an arthroscopic rotator cuff repair the biceps tendon is often treated (Mardani-Kivi et al 2019). The orthopedic literature is starting to recognize the importance of addressing the biceps brachii lesions when the co-occur, although the surgical literature for the treatment both of these tendons at the same time remains limited (Gartsman et al 1998; Streit et al 2015).
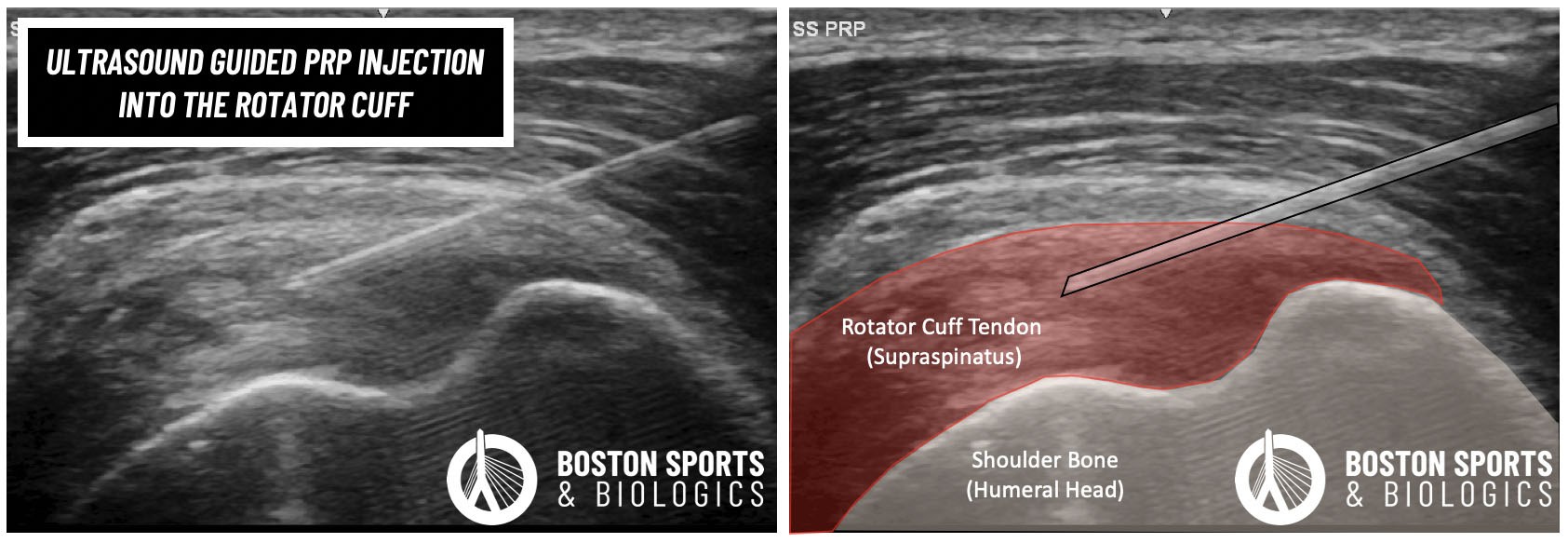
Case Study: Treating both the rotator cuff and biceps brachii tendon?
Orthobiologic injections have to be accurately placed into the involved tendon, and one reason that PRP injections fail in the shoulder is that co-occurring tendon injuries are missed. In this case, the patient had a partial rotator cuff tear and an interstitial tear of the long head of the biceps brachii tendon. Ultrasound was used to confirm the location of pain and accurately place the PRP injection into both tendons.
Orthobiologic injections have to be accurately placed into the involved tendon, and one reason that PRP injections fail in the shoulder is that co-occurring tendon injuries are missed. In this case below, the patient had a partial rotator cuff tear and an interstitial tear of the long head of the biceps brachii tendon. Ultrasound was used to confirm the location of pain and accurately place the PRP injection into both tendons.
At Boston Sports & Biologics, we use diagnostic ultrasound and differential injections to confirm the location of the shoulder pain. Boston Sports & Biologics is one of the few clinics in Massachusetts to be accredited by the American Institute of Ultrasound Medicine (AIUM) in diagnostic musculoskeletal ultrasound and ultrasound guided injections. Orthobiologics is a new field and successful placement of these injections into the tendon matters. Make sure you confirm that your physician is adequately trained to place these injections.
Learn how ultrasound-guided percutaneous fasciotomy may revolutionize treatment for chronic exertional compartment syndrome with faster recovery and smaller incisions.
Read MoreResearchers used artificial intelligence and natural language processing to identify Shoulder Injury Related to Vaccine Administration (SIRVA) cases from over 3.7 million vaccinations. Learn what the study found, how
Read More