The rotator cuff is a group of four muscles and associated tendons are crucial to stabilizing the shoulder joint and facilitating arm movements.
During arm movements, the rotator cuff muscles work together to keep the head of the humerus firmly within the shallow socket of the shoulder blade (glenoid cavity). They act as dynamic stabilizers, counteracting the forces generated by larger muscles like the deltoid, which can cause superior translation of the humeral head.
This coordinated action is essential for maintaining shoulder stability and allowing a wide range of motion.
The rotator cuff includes the supraspinatus, infraspinatus, subscapularis, and teres minor muscles/tendons.
Supraspinatus: This muscle is located at the top of the shoulder and is primarily responsible for initiating arm abduction. It also helps stabilize the humerus's head in the glenoid cavity during arm movements.
Infraspinatus: Situated below the supraspinatus, this muscle is involved in external shoulder rotation and contributes to the stabilization of the shoulder joint.
Subscapularis: This is the largest and strongest muscle of the rotator cuff, located on the anterior surface of the scapula. It is responsible for internal rotation of the shoulder and plays a significant role in maintaining the stability of the shoulder joint.
Teres Minor: This small muscle is located below the infraspinatus and assists in external rotation and adduction of the arm. It also contributes to the stabilization of the shoulder joint.
What is a Rotator Cuff tear?
A rotator cuff tear is a common shoulder injury involving damage to one or more of the tendons that make up the rotator cuff.
Partial-Thickness Tears: These involve damage to some
of the tendon fibers without completely severing the tendon. They are
often associated with early degenerative changes and can progress to
full-thickness tears if left untreated.
Studies have shown that partial-thickness tears exhibit significant
tendon degeneration, including increased cellularity, vascularity, and
stainability [Jo et al, 2017].
Full-Thickness Tears: These involve a complete tear through the tendon, leading to significant functional impairment.
Full-thickness tears are associated with more advanced degenerative
changes and can lead to rotator cuff tear arthropathy, characterized by
superior migration of the humeral head and arthritis over time [Jain & Khazzam, 2024].
What causes a Rotator Cuff Tear?
The pathophysiology of rotator cuff tears involves a complex interplay of intrinsic and extrinsic factors leading to tendon degeneration and eventual tearing.
Intrinsic Factors/Degeneration: These include age-related degeneration, vascular insufficiency, and genetic predisposition.
Chronic wear and tear, often seen in individuals over 40 years of age, can lead to tendon degeneration and subsequent tearing.
Risk factors include repetitive overhead activities, heavy manual labor, smoking, andcertain comorbidities like diabetes and hypercholesterolemia [Hashimoto et al, 2003; Prasetia et al, 2023].
Degenerative changes within the tendon, such as matrix disorganization, myxoid degeneration, and fatty infiltration, are common.
Histopathologic studies have shown thinning and disorientation of
collagen fibers, myxoid degeneration, and hyaline degeneration as early
degenerative processes [Hashimoto et al, 2003].
Oxidative stress and unregulated autophagy also contribute to tendon degeneration, particularly in chronic tears [Prasetia et al, 2023].
Extrinsic Factors/Trauma:
These include mechanical impingement, repetitive overhead activities,
and acute trauma.
Acute injuries such as falls, motor vehicle accidents, or heavy lifting can cause tears.
Even a simple fall can cause an acute rotator cuff tear due
to sudden eccentric loading of the tendon-muscle unit [Nyffeler et al, 2021].
Are there different types of Rotator Cuff tears?
Rotator cuff disorders represent a continuum of tendon damage, ranging from mild to severe.
This spectrum includes rotator cuff tendinopathy, partial-thickness tears, full-thickness tears, and, at the most advanced stage, rotator cuff tear arthropathy—a condition characterized by chronic tendon rupture, upward displacement of the humeral head, and progressive joint degeneration.
Types of Tears:
Partial-Thickness Tears: Partial-thickness tears involve damage to some of the tendon fibers without completely severing the tendon. These tears can progress to full-thickness tears if left untreated.
Full-Thickness Tears: Full-thickness tears, on the other hand, involve a complete tear through the tendon, leading to significant functional impairment.
A comprehensive review in The Journal of the American Academy of Orthopaedic Surgeons discusses the diagnosis and management of partial-thickness rotator cuff tears, emphasizing the importance of early diagnosis and appropriate treatment to prevent progression to full-thickness tears [Plancher et al, 2021].
What are the symptoms of a rotator cuff injury?
Common symptoms of a rotator cuff tear includes:
Pain at rest or at night: This is often worse when lying on the affected shoulder, leading to sleep disturbances.
The American Medical Society for Sports Medicine highlights that night pain is a dominant feature in both gradual onset tendinopathy and acute tears, often exacerbated by lying on the affected shoulder [Kibler & Putukian, 2010].
Pain with arm movements: Pain is typically felt when lifting or lowering the arm, especially during overhead activities or reaching behind the back.
Weakness: There is often noticeable weakness when lifting or rotating the arm, which can affect daily activities.
Localized pain: Pain is usually felt over the outside of the shoulder but can also occur over the front or back of the shoulder.
However, in one study in the Journal of Shoulder and Elbow Surgery, this number was higher wit: 65.4% of individuals with rotator cuff tears being asymptomatic [Yamamoto et al, 2011].
How do you know if you have a Rotator Cuff Tear?
The combination of clinical presentation, physical examination, and imaging modalities such as MRI, US, and MRA provides a comprehensive approach to diagnosing rotator cuff tears.
Clinical Presentation:
Patients typically present with insidious onset of lateral shoulder
pain, which may worsen at night and lead to sleep disturbances. Pain is
often exacerbated by overhead activities or reaching behind the back.
Weakness in lifting the arm above shoulder level is common [Jain & Khazzam, 2024].
Physical Examination:
The examination includes inspection for muscle atrophy, assessment of
scapular posture, and shoulder asymmetry. Active range of motion and arm
strength in abduction, forward flexion, and external rotation are
usually affected. Passive range of motion may be normal but limited by
pain.
Specific maneuvers can help diagnose a torn rotator cuff, although their
sensitivities and specificities vary [Jain & Khazzam, 2024]. Combining multiple clinical tests increases diagnostic accuracy, as no single test is sufficiently reliable on its own [Lädermann et al, 2021].
Imaging: In addition to clinical presentation and physical examination, imaging modalities play a crucial role in diagnosing rotator cuff tears.
Radiographs:
While not used to diagnose rotator cuff tears directly, radiographs can
identify other sources of shoulder pain and provide information on
chronic tears, such as proximal humeral head migration and loss of the
acromiohumeral interval [Jain & Khazzam, 2024].
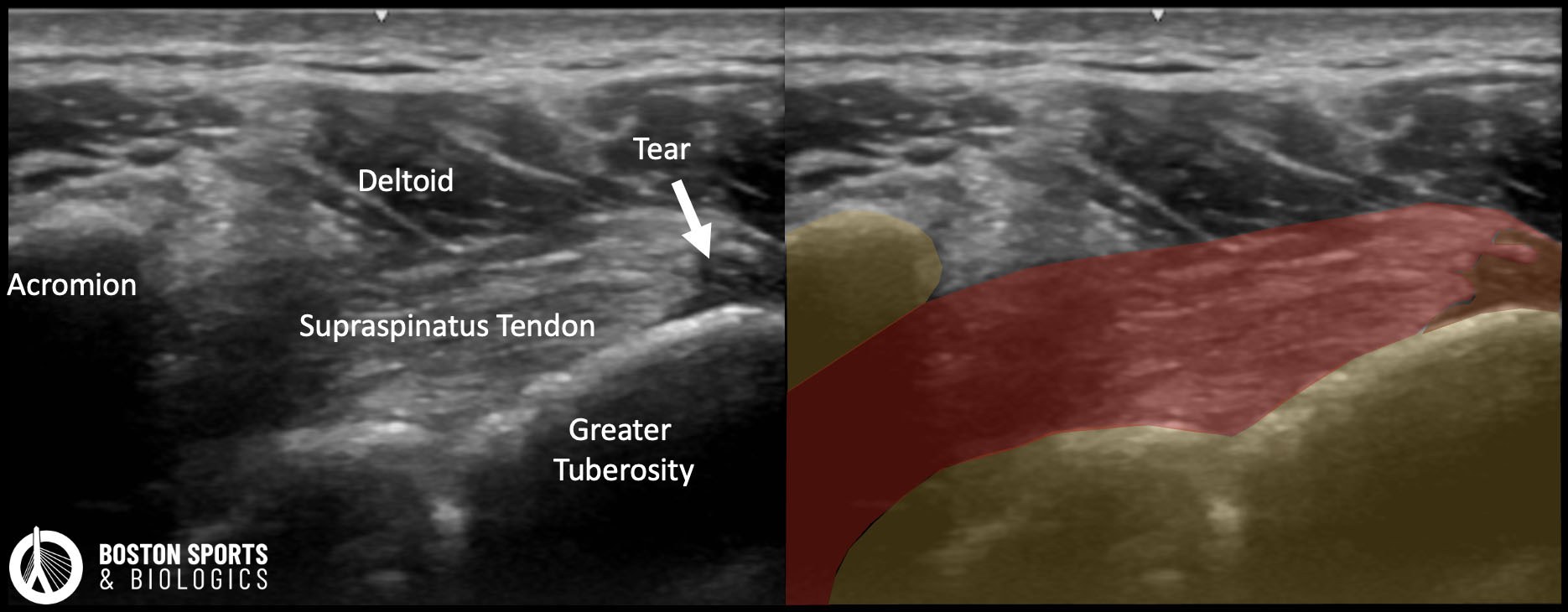
Ultrasonography and MRI: MRI and US are both effective for diagnosing rotator cuff tears. These imaging modalities can confirm rotator cuff tears and provide
detailed information on the size, location, tendon retraction, muscle
atrophy, and fatty infiltration. The choice between these modalities may depend on clinical context, availability, and the need for detailed anatomical information.
MRI is considered the gold standard for evaluating rotator cuff pathology [Jain & Khazzam, 2024]. It provides comprehensive information on the size and location of tears, tendon retraction, muscle atrophy, and fatty infiltration.
MRI has high sensitivity and specificity for diagnosing full-thickness rotator cuff tears, with a sensitivity of 94% and specificity of 93% [Lenza et al, 2013].
However, its diagnostic accuracy for partial-thickness tears is lower, and incidental findings can occur when MRI is performed for other indications [Zoga et al, 2021].
Ultrasound (US) is a cost-effective, portable, and dynamic imaging modality that can be performed at the point of care.
It has similar sensitivity and specificity to MRI for diagnosing full-thickness rotator cuff tears, with a sensitivity of 91% and specificity of 85% [Lenza et al, 2013].
US is advantageous in settings where quick, real-time imaging is needed, and it can be a cost-effective alternative to MRI.
However, US is operator-dependent, and because of this its accuracy can be lower for partial-thickness tears with inexperienced operators.[Zoga et al, 2021]. Additionally, US may have limitations in evaluating deeper structures and in patients with a high body mass index.
A meta-analysis in the American Journal of Roentgenology found no significant differences in sensitivity or specificity between MRI and US for diagnosing partial- or full-thickness rotator cuff tears [de Jesus et al, 2009].
Another study in PLoS One reported that high-resolution US and MRI showed moderate to almost perfect agreement in assessing a wide range of shoulder joint pathologies, including rotator cuff tears [Wengert et al, 2019].
What are the Treatment options for a Rotator Cuff Tear?
Treatment options for a rotator cuff tear include both conservative and surgical methods, with each treatment having certain indications and evidence supporting its use.
Conservative Treatments:
Physical Therapy: Physical therapy is a cornerstone of nonoperative treatment, focusing on restoring range of motion, addressing stiffness, and strengthening the rotator cuff and scapular muscles. Studies have shown that more than 80% of patients report reduced pain and improved function after supervised physical therapy [Jain & Khazzam, 2024].
Medications: Nonsteroidal anti-inflammatory drugs (NSAIDs) and acetaminophen are commonly used to manage pain and inflammation. The American Medical Society for Sports Medicine recommends acetaminophen as the first-line pharmacologic treatment, with NSAIDs considered if acetaminophen is ineffective [Kibler & Putukian, 2010].
Corticosteroid Injections: These are used for short-term symptom relief.
Multiple randomized controlled trials found that corticosteroid injections only provides short term pain relief [Jo et al, 2020; Wang et al, 2021].
Platelet-Rich Plasma (PRP) Injections: PRP is an autologous blood product rich in platelets, growth factors, and cytokines, which may enhance tendon healing and reduce inflammation.
PRP injections have been shown to provide better medium- to long-term improvements in function and pain compared to corticosteroid injections [Jo et al, 2020; Wang et al, 2021].
Evidence from multiple systematic reviews and meta-analyses concluded that PRP is a viable alternative to corticosteroids, with fewer post-injection failures and better long-term outcomes [Pang et al, 2023; Hamid et al, 2021; Chen et al, 2020].
While PRP injections are generally safe, their efficacy can vary based on the bioformulation, including factors such as leukocyte concentration and gel vs. nongel [Chen et al, 2020].
Overall, PRP injections represent a viable alternative to corticosteroid injections for conservative treatment of rotator cuff disease, offering potential advantages in pain relief and functional recovery [Hamid et al, 2021; Chen et al, 2020].
Mesenchymal stem cells (MSCs) or stromal cells are derived from bone marrow or adipose tissue have shown potential in promoting tendon healing.
A review in the International Journal of Molecular Sciences highlighted
that mesenchymal stem cells can reduce inflammation, improve tissue remodeling, and
enhance tendon strength in animal models.
Human trials suggest that mesenchymal stem cells might lower retear rates and improve
post-repair outcomes, but results are mixed, and more rigorous clinical
trials are needed to confirm their efficacy [Hooper et al, 2024].
Bone Marrow Aspirate Concentrate (BMAC): BMAC is rich in mesenchymal stem cells and growth factors, which may enhance tendon healing.
A systematic review in Arthroscopy found that BMAC may improve healing rates, pain relief, and functional outcomes in rotator cuff repair, although the evidence is heterogeneous [Carola et al, 2024].
A randomized controlled trial in The American Journal of Sports Medicine reported that BMAC-augmented arthroscopic rotator cuff repair resulted in a structurally superior repair with lower retear rates (18% vs. 57% in the control group) but did not significantly improve patient-reported outcomes [Cole et al, 2023].
Micro-Fragmented Adipose Tissue (MFAT): MFAT is a source of non expanded adipose-derived MSCs.
A randomized controlled trial in The American Journal of Sports Medicine demonstrated that MFAT injection during arthroscopic rotator cuff repair improved short-term clinical and functional outcomes without increasing complication rates [Randelli et al, 2022].
Surgical Interventions:
Arthroscopic surgery is commonly used to treat both full-thickness and partial-thickness rotator cuff tears. While minimally invasive, it still general anesthesia and a long recovery period—and outcomes can vary, particularly in cases of partial-thickness tears.
Full-Thickness Tears involve complete tendon detachment, often requiring surgical reattachment with suture anchors. Studies show significant improvements in pain and function, especially in younger patients. However, retear rates can rise over time with failure rates and retear rates for full-thickness rotator cuff tears varying based on several factors, including tear size, tendon quality, and patient characteristics.
A study in The Journal of Bone and Joint Surgery reported an increase in retear rates from 10% at six months to 20% by 24 months [Peters et al, 2012].
A systematic review in The American Journal of Sports Medicine reported that the retear rate for arthroscopic rotator cuff repair (aRCR) of full-thickness tears was approximately 43% at long-term follow-up, with no significant difference compared to open/mini-open repairs [Plachel et al, 2023].
Another study in Arthroscopy found that the retear rate between 1 and 2 years postoperatively was 33.3% for patients with higher tear size and fatty degeneration [Akimoto et al, 2024]. Factors influencing retear rates include the size of the tear, tendon quality, and the presence of fatty degeneration.
A study in The American Journal of Sports Medicine identified that larger tear size, greater fatty infiltration, and older age were significant predictors of retears, with an overall retear rate of 27% for full-thickness tears [Le et al, 2014].
Partial-Thickness Tears involve only a portion of the tendon, but can be complex to manage surgically.
Arthroscopic techniques for these tears include in situ transtendon repair (which preserves the remaining intact tendon fibers), tear completion and repair (which converts the tear to a full-thickness defect for reattachment), and debridement (removal of damaged tissue without full repair).
In situ repair while tissue-preserving, is technically demanding and can risk overtightening the tendon or causing residual pain.
Tear completion and repair although allowing for a more straightforward repair, involves intentionally extending the injury to convert it into a full-thickness tear prolonging healing.
Debridement removes damaged tissue and is least invasive, but may not adequately address underlying biomechanical dysfunction, leading to recurrence or progression of symptoms.
The retear rate for arthroscopic repairs of partial-thickness rotator cuff tears are generally lower than those observed for full-thickness tears, reflecting the relatively better prognosis for partial-thickness tear repairs. The retear rate varies based on the specific surgical technique and patient factors.
According to a meta-analysis in The American Journal of Sports Medicine, the retear rate for partial-thickness rotator cuff tears repaired arthroscopically is approximately 6.8% to 9.5% [Dalmas et al, 2025].
Another study in The Journal of Bone and Joint Surgery reported a retear rate of 5% at six months, increasing to 10% at twenty-four months postoperatively [Peters et al, 2012].
Theevidence for debridement and subacromial decompression does not provide clinically important benefits over placebo in terms of pain, function, or quality of life for partial rotator cuff tears.
A Cochrane review of eight trials (1,062 participants) assessed subacromial decompression surgery for rotator cuff disease (excluding full-thickness tears). Two trials comparing the surgery to placebo (arthroscopy only) and found no significant improvement in pain, function, or quality of life up to one year post-op. Pain scores improved by just 0.26 points (95% CI: 0.84 better to 0.33 worse), and function scores by 2.8 points (95% CI: 1.4 worse to 6.9 better) [Karjalainen et al, 2019].
A multicenter placebo-controlled trial (CSAW) published in The Lancet found no added benefit of arthroscopic subacromial decompression over placebo surgery for subacromial shoulder pain. Both surgical groups showed only minor, clinically insignificant improvements over no treatment. At six months, the Oxford Shoulder Score difference between decompression and placebo was -1.3 points (95% CI: -3.9 to 1.3) [Beard et al, 2018].