Email: info@BSBortho.com
While there are several types of arthritis that can affect the hip, osteoarthritis (OA) is degenerative and occurs when the protective cartilage that cushions the end of the bones wears down with time.
Hip osteoarthritis, is one of the most common joint disorders in the United States. Based on population studies, 19.6% of people over the age of 50 have radiographic evidence of hip OA and 4.2% have symptomatic disease (Kim et al, 2014).
Several risk factors may contribute to the development of hip OA, including:
Systemic risk factors (e.g. age, gender, genetics)
Intrinsic joint risk factors (e.g. anatomic variants and joint laxity)
Extrinsic risk factors (e.g. repetitive physical activities and obesity)
Population studies suggest that hip OA is twice as common in women as in men, and there is evidence to suggest a strong genetic component (Aresti et al, 2016), however, to date the exact primary hip OA etiology remains unknown (Lespasio et al, 2018).
The degenerative process in osteoarthritis effects the entire joint, and involves a progressive loss of articular cartilage, subchondral cystic formation, osteophyte or bone spur formation, periarticular ligamentous laxity, muscle weakness, and possible synovial inflammation (Hutton et al, 1989).
As the cartilage cushion wears down the cartilage becomes rough, and patients may experience clicking and decreased range of motion.
The diagnosis of hip osteoarthritis is based on a detailed history, physical examination, and imaging.
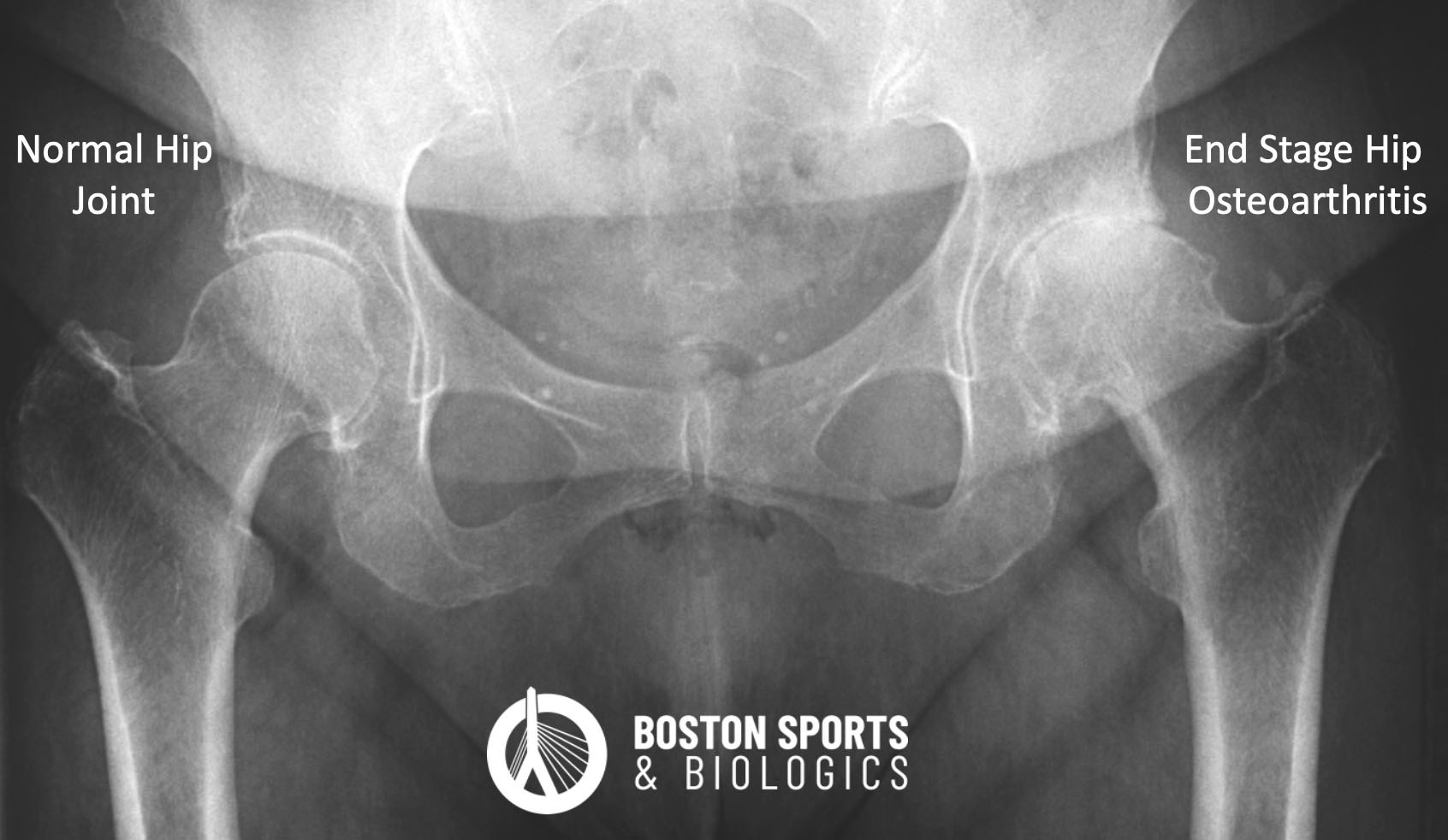
Plain radiographs or x-rays are the most common modality to diagnose hip osteoarthritis, and can show features of cartilage damage including narrowing of the joint, bone cysts and bone spurs (osteophytes) (Aresti et al, 2016; Karachalios et al, 2007). However, there is a difference between clinical symptoms of arthritis and radiographic findings of arthritis.
Only 21% of patients with hip osteoarthritis experience pain. With such a high risk of incidental radiographic findings, patients may undergo unnecessary treatments that will not improve their symptoms, an accurate diagnosis is important to guide treatment decisions (Kim et al, 2015).
Hip pain from osteoarthritis can be confused with other common hip conditions, including greater trochanteric pain syndrome, piriformis syndrome, adductor tendon pain, stress fracture, inflammatory arthropathies (e.g. rheumatoid arthritis), lumbar radiculopathy, pelvis bone tumors, osteonecrosis, pelvic insufficiency fractures, and meralgia parasthetica. Non-musculoskeletal conditions (e.g. groin hernia, intrapelvic pathology, and leaking abdominal aortic aneurysms) may also present with hip and/or groin pain.
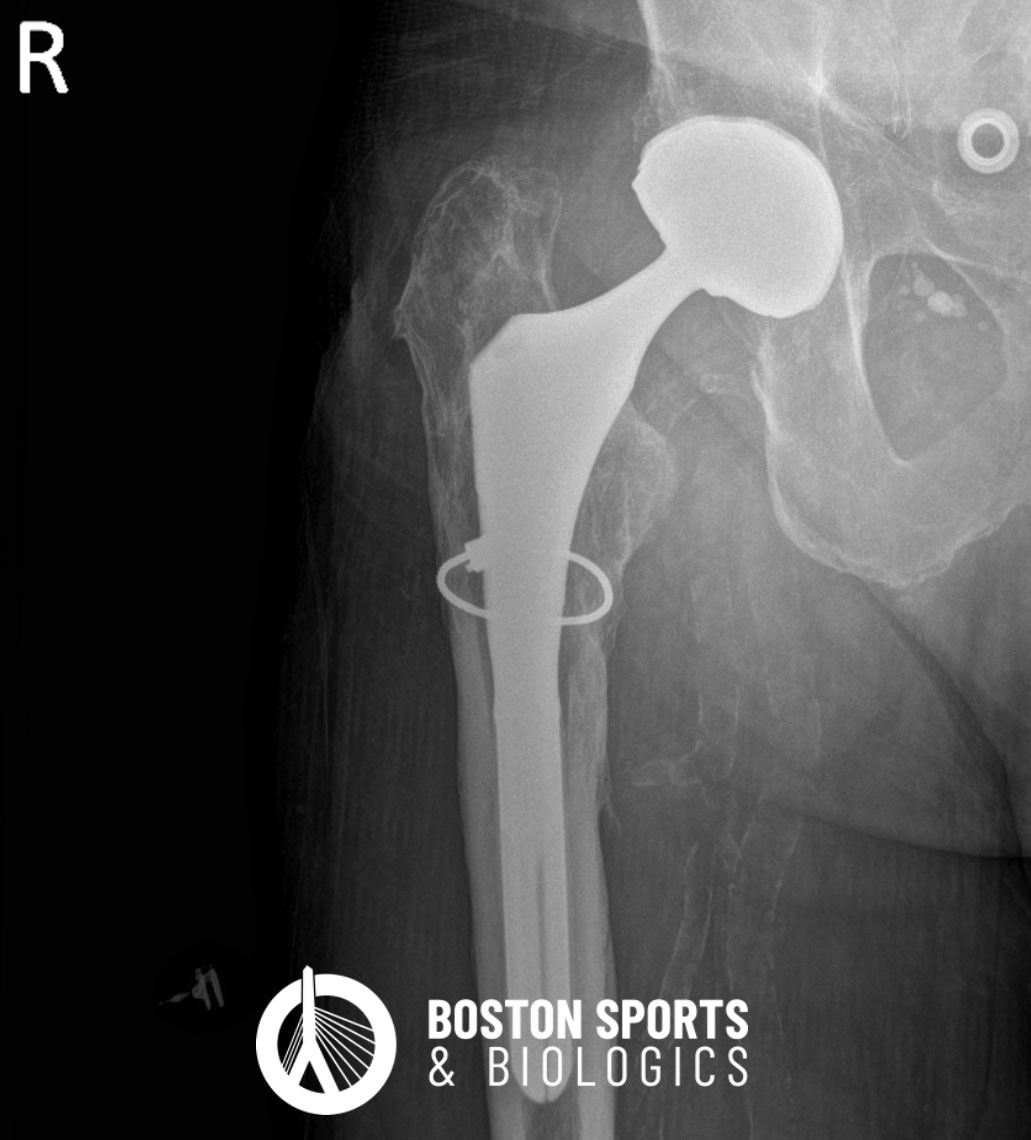
Surgical Management
References