Email: info@BSBortho.com
Chronic groin pain can be one of the most frustrating injuries for athletes and active individuals. It often lingers despite rest, physical therapy, and injections—and when it doesn’t improve, treatment options historically jump straight from conservative care to open surgery.
For patients with chronic adductor longus tendinopathy, a newer option is emerging: ultrasound-guided tenotomy using the Tenex system. Recent clinical evidence suggests this minimally invasive approach may effectively relieve pain, restore function, and allow a faster return to sport—without the morbidity of traditional surgery.
The adductor longus is one of the most commonly injured tendons in the groin. While acute adductor strains often resolve with rehabilitation, chronic adductor-related groin pain behaves differently. Learn more about core injuries here.
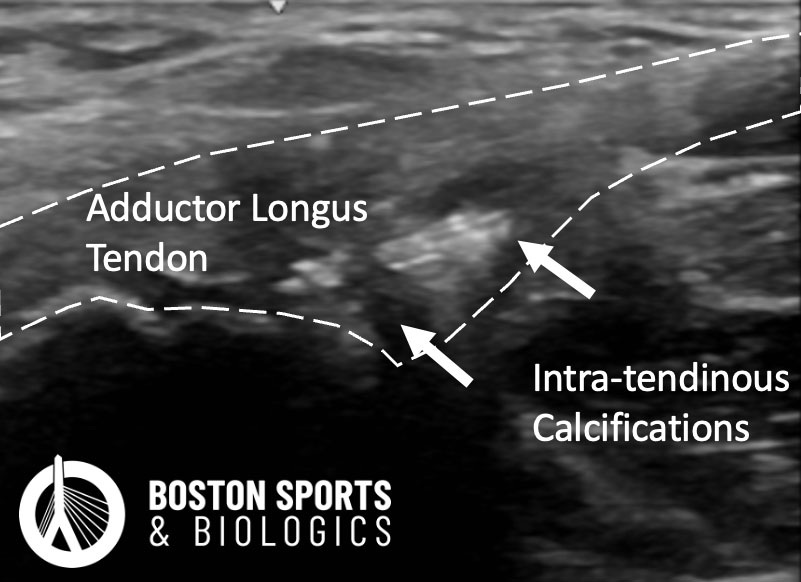
Research shows that chronic adductor longus tendinopathy is degenerative rather than inflammatory. Instead of active inflammation, the tendon demonstrates:
Collagen disorganization
Mucoid degeneration
Poor vascularity
Microtearing at the pubic attachment
These changes limit the tendon’s ability to heal on its own, which explains why rest, anti-inflammatory treatments, and repeated physical therapy may fail [Khan et al, 1999].
When conservative care fails, surgical options such as open or partial adductor tenotomy have traditionally been considered. There is no consensus in the literature regarding the optimal surgical approach. Learn more about surgical approaches to adductor longus pathology here.
Both “partial” and “total tenotomy” techniques offer similar efficacy for pain relief. However, studies have demonstrated that a complete tenotomy of the adductor longus tendon may relieve symptoms, but at the expense of strength, with variable outcomes upon return to sport.
Tenex is a minimally invasive procedure that uses a specialized microtip to:
Precisely cut and remove degenerative tendon tissue
Preserve healthy tendon fibers
Stimulate the body’s natural healing response
The procedure is performed under real-time ultrasound guidance, allowing the physician to directly visualize the tendon, avoid nearby nerves and vessels, and target only the diseased tissue.
Importantly, Tenex acts as a tissue-preserving debridement, making it particularly attractive for athletes concerned about strength and performance. Learn more about Tenex here.
Not all minimally invasive adductor tendon releases are the same. Landmark-guided procedures rely on surface anatomy rather than real-time visualization, which means the surgeon cannot directly see the tendon or the surrounding structures during the procedure.
This is important because several critical structures run very close to the adductor longus tendon. In men, the spermatic cord lies just above the tendon; in women, the round ligament follows a similar path. Nearby nerves that supply sensation to the groin region also pass within one to two centimeters of the tendon attachment. Because of this close proximity—and because anatomy varies significantly from person to person—there is no consistently reliable “safe zone” for blind or landmark-based procedures. [O'Donnell et al, 2023; Capurro et al, 2024; Santamaria-Le Pera, 2025].
Techniques that allow direct visualization of the tendon, such as endoscopic or ultrasound-guided approaches, may reduce these risks. Ultrasound, in particular, is already well established as a tool for diagnosing adductor longus tendinopathy. However, ultrasound-guided release of the adductor longus tendon is not always offered.
Compared with traditional surgical approaches, Tenex offers several potential benefits:
Minimally invasive ultrasound-guided technique
Local anesthesia only (no general anesthesia)
Real-time ultrasound precision
For appropriately selected patients, Tenex may function as an intermediate treatment option—more targeted than injections, but far less disruptive than open surgery.
Chronic adductor longus tendinopathy is a challenging condition that often resists traditional treatment. Ultrasound-guided Tenex tenotomy offers a promising, evidence-supported alternative that targets the underlying degenerative tendon pathology while minimizing risk and downtime.
As clinical experience and research continue to expand, Tenex may become a key part of the treatment algorithm for athletes and active individuals seeking durable relief from chronic groin pain—without sacrificing performance
Tenex is a minimally invasive, ultrasound-guided procedure used to treat chronic tendon pain by precisely removing damaged tissue while preserving healthy tendon fibers. It is particularly useful for patients with chronic adductor longus tendinopathy that has not improved with physical therapy or injections
Tenex uses a specialized cutting device to:
This is important because chronic tendinopathy is degenerative (not inflammatory), meaning the damaged tissue often needs to be removed to allow proper healing
You may be a candidate if you have:
Tenex is often ideal for patients looking to avoid traditional surgery but need more than conservative care.
Tenex is not necessarily “better” for every patient, but it offers key advantages:
Traditional open or full tenotomy procedures may relieve pain but can result in strength loss and longer downtime, while Tenex targets only the diseased tissue
Recovery is typically faster than surgery:
Rehabilitation is still important to optimize outcomes.
For many patients, Tenex can:
It is often considered before surgical intervention in chronic cases.
If symptoms persist, additional options may include:
However, Tenex does not “burn bridges”—it preserves anatomy, so future treatments remain available.
Tenex is often used when injections alone are not enough.
Coverage varies depending on your plan.
An adductor longus tenotomy is a procedure where part or all of the adductor tendon is released to relieve chronic groin pain. It is commonly used in athletes with adductor-related groin pain or sports hernia–type injuries when conservative treatment fails.
Selective tenotomy is designed to reduce pain while maintaining strength and stability, whereas full release may relieve pain but can lead to weakness and longer recovery
Evidence and clinical experience suggest that selective tenotomy often leads to faster recovery and better functional outcomes. Athletes undergoing targeted procedures can return to sport sooner compared to full releases
Additionally, modern surgical approaches focused on preserving anatomy show high return-to-sport rates (often >90%)
Return to play varies depending on the procedure:
Some studies report return to sport around 9–12 weeks on average after surgery, depending on the athlete and associated procedures
Potentially, yes. Full adductor release can:
Selective approaches aim to preserve strength and athletic performance, which is why they are increasingly favored.
You may be a candidate if you have:
Surgery is typically considered only after conservative care has failed.
No. First-line treatment includes:
Surgery is reserved for persistent, high-level symptoms, particularly in athletes.
Surgical treatment of adductor-related groin pain has shown:
However, outcomes are best when the procedure is targeted to the correct pain generator.
Potential risks include:
Serious complications are uncommon, especially with modern techniques.
Recovery typically includes:
Selective procedures often allow for faster and more predictable rehabilitation.
Modern sports medicine is shifting toward tissue-preserving approaches. Selective tenotomy:
This aligns with broader trends toward minimally invasive and function-preserving treatments.
Åkermark C and Johansson C. Tenotomy of the adductor longus tendon in the treatment of chronic groin pain in athletes. The American Journal of Sports Medicine 1992; 20: 640 - 643-640 - 643. DOI: 10.1177/036354659202000604.
Atkinson H, Parminder J, Falworth M, et al. Adductor tenotomy: its role in the management of sports-related chronic groin pain. Archives of Orthopaedic and Trauma Surgery 2010; 130: 965-970-965-970. DOI: 10.1007/s00402-009-1032-4.
Capurro B, Chapman RS, Kaplan DJ, et al. The Genitofemoral Nerve Is the Structure Closest to the Tendon Footprint and Is Most at Risk for Iatrogenic Injury During Proximal Adductor Longus Repair: A Cadaveric Anatomy Study. Arthroscopy, Sports Medicine, and Rehabilitation 2024; 6: 100970. DOI: https://doi.org/10.1016/j.asmr....
Khan KM, Cook JL, Bonar F, et al. Histopathology of common tendinopathies. Update and implications for clinical management. Sports Med 1999; 27: 393-408. DOI: 10.2165/00007256-199927060-00004.
Maffulli N, Loppini M, Longo U, et al. Bilateral Mini-Invasive Adductor Tenotomy for the Management of Chronic Unilateral Adductor Longus Tendinopathy in Athletes. The American Journal of Sports Medicine 2012; 40: 1880 - 1886-1880 - 1886. DOI: 10.1177/0363546512448364.
O'Donnell R, DeFroda S, Bokshan SL, et al. Cadaveric Analysis of Key Anatomic Structures of Athletic Pubalgia. J Am Acad Orthop Surg Glob Res Rev 2023; 7 20230614. DOI: 10.5435/JAAOSGlobal-D-23-00070.
Robertson IJ, Curran C, McCaffrey N, et al. Adductor Tenotomy in the Management of Groin Pain in Athletes. International Journal of sports Medicine 2010; 32: 45 - 48-45 - 48. DOI: 10.1055/s-0030-1263137.
Santamaría-Le Pera J, Valera-Garrido F, Valderrama-Canales FJ, et al. Are palpation-guided interventional procedures on the adductor longus muscle safe? A cadaveric and sonographic investigation. Surg Radiol Anat 2025; 47: 74. 20250207. DOI: 10.1007/s00276-025-03567-2.
Learn how ultrasound-guided percutaneous fasciotomy may revolutionize treatment for chronic exertional compartment syndrome with faster recovery and smaller incisions.
Read MoreResearchers used artificial intelligence and natural language processing to identify Shoulder Injury Related to Vaccine Administration (SIRVA) cases from over 3.7 million vaccinations. Learn what the study found, how
Read More