Email: info@BSBortho.com
Shoulder pain after a vaccine is usually mild and temporary. However, in rare cases, patients may develop persistent shoulder pain and loss of motion due to a condition known as Shoulder Injury Related to Vaccine Administration (SIRVA).
In our recent case series published in Clinical Journal of Sport Medicine we describe ultrasound finding within the rotator cuff tendons that may help diagnose SIRVA and guide targeted treatment [Sussman et al. 2026].
Understanding this condition is important for patients who develop ongoing shoulder pain after vaccination that does not improve with typical treatments.
Shoulder Injury Related to Vaccine Administration (SIRVA) is a rare vaccine-related complication that occurs when a vaccine is inadvertently injected too high or too deep into the shoulder (learn more here). Instead of entering the deltoid muscle, vaccine material may reach deeper structures such as:
Rotator cuff tendons
Subacromial bursa
Shoulder joint capsule
Bone near the greater tuberosity
This can trigger an inflammatory or immune-mediated reaction that causes pain and restricted motion [National Academies of Sciences].
Symptoms typically develop within 24–48 hours after vaccination and persist longer than expected for normal injection soreness [National Academies of Sciences].
Common symptoms include:
Persistent shoulder pain
Difficulty lifting the arm
Pain with overhead activity
Night pain
Reduced range of motion
SIRVA is estimated to occur in less than 1% of vaccine administrations, but awareness has increased in recent years [de Lusignan et al, 2020].
Historically, imaging studies such as MRI have been used to evaluate persistent shoulder pain after vaccination. MRI findings may include:
Subacromial bursitis
Rotator cuff tendinopathy or tears
Adhesive capsulitis (frozen shoulder)
Bone inflammation
These findings are nonspecific and overlap with common shoulder conditions [National Academies of Sciences]. Because of this, diagnosing SIRVA can sometimes be challenging.
Musculoskeletal ultrasound is increasingly used to evaluate shoulder injuries because it allows physicians to visualize tendons dynamically and perform diagnostic injections during the same visit.
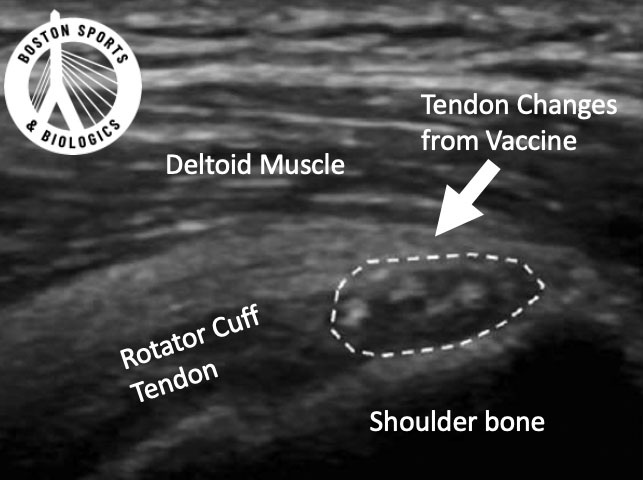
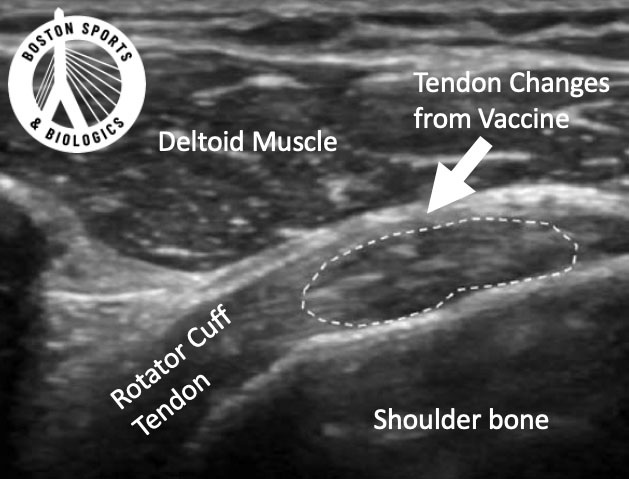
Our recent case series identified a distinct ultrasound pattern in patients with persistent SIRVA symptoms. All patients demonstrated a unique ultrasound appearance in the rotator cuff tendons characterized by:
Multiple punctate hyperechoic foci within the tendon tissue arranged in a disorganized pattern. These bright spots were:
Less than 1 mm in size
Located within the supraspinatus or infraspinatus tendons
Not associated with acoustic shadowing
Distinct from degenerative tendon disease
This pattern had not previously been described in the SIRVA literature, and may represent reactive intratendinous fibrosis or inflammatory changes caused by vaccine exposure to the tendon.
Because imaging findings alone do not always prove the sourceof symptoms, we take an additional diagnostic step.
An ultrasound-guided anesthetic injections directly into the abnormal tendon region can help confirm the source of pain. After the anesthetic injection, patients are then asked to perform movements that previously caused pain.
A positive test is defined as greater than 80% pain relief, which confirmed that the abnormal tendon area was the pain generator.
After confirming the diagnosis, patients are offered a minimally invasive ultrasound-guided procedure using the Tenex device to perform a tenotomy with vacuum aspiration and debridement. Learn about the procedure here.
This technique uses a specialized device (Tenex MicroTip) that:
Breaks up abnormal tendon tissue
Aspirates inflammatory debris
Stimulates healing of the tendon
The procedure is performed through a small skin incision using ultrasound guidance.
This technology has previously been used to treat chronic tendinopathy in other areas of the body
Our study followed patients for an average of 16.2 months after treatment [Sussman et al. 2026].
Key findings included:
Significant improvements in shoulder pain
Improved function and activity tolerance
High patient satisfaction
Pain was measured using the Numeric Rating Scale (NRS) and functional outcomes were assessed using the QuickDASH questionnaire.
Most patients experienced substantial improvement after the procedure.
Two patients required additional treatments for associated shoulder conditions:
One had a rotator cuff tear that later received PRP treatment
Another required treatment for adhesive capsulitis
Despite these additional conditions, the majority of patients experienced sustained pain relief and improved shoulder function.
This study expands our understanding of SIRVA in several important ways.
The identification of punctate hyperechoic tendon lesions may provide clinicians with a new imaging clue when evaluating persistent shoulder pain after vaccination.
Using ultrasound with diagnostic anesthetic injections can help confirm the true source of pain.
Identifying a specific tendon abnormality allows physicians to perform targeted minimally invasive procedures rather than relying solely on conservative care.
Most vaccine-related shoulder soreness improves within a few days.
However, patients should seek evaluation if they experience:
Severe shoulder pain within 24–48 hours after vaccination
Pain lasting longer than 1–2 weeks
Difficulty raising the arm
Night pain or persistent stiffness
Limited shoulder motion
Early evaluation can help determine whether symptoms represent normal soreness or a more significant shoulder injury.
High-resolution musculoskeletal ultrasound is becoming a powerful tool for diagnosing shoulder injuries.
Advantages include:
Real-time imaging
Ability to perform diagnostic injections
Lower cost than MRI
Dynamic evaluation during movement
For conditions like SIRVA, ultrasound may provide critical diagnostic information that cannot always be seen on MRI alone.
Shoulder Injury Related to Vaccine Administration (SIRVA) is a rare but important cause of persistent shoulder pain after vaccination.
New research demonstrates that ultrasound may reveal a unique tendon pattern consisting of punctate hyperechoic foci, which can help identify the source of pain and guide treatment.
When confirmed with a diagnostic injection, ultrasound-guided minimally invasive procedures may provide meaningful relief for patients whose symptoms do not improve with conservative care.
Yes. Mild shoulder soreness is a common side effect after vaccination and usually resolves within a few days. This type of discomfort occurs because the immune system reacts to the vaccine in the deltoid muscle. However, if shoulder pain is severe, limits arm movement, or lasts longer than a week, it may indicate a different problem such as Shoulder Injury Related to Vaccine Administration (SIRVA).
SIRVA is a rare complication that occurs when a vaccine is injected too high or too deep into the shoulder rather than the deltoid muscle. The injection can affect structures such as the rotator cuff tendons, subacromial bursa, or joint capsule, leading to inflammation, pain, and reduced shoulder mobility.
Symptoms of SIRVA usually begin within 24–48 hours after vaccination. Patients often report persistent shoulder pain, difficulty lifting the arm, and pain with overhead activities that do not improve with typical post-vaccine soreness treatments.
Doctors diagnose SIRVA based on a combination of medical history, physical examination, and imaging tests. Imaging studies such as ultrasound or MRI may reveal findings such as bursitis, rotator cuff inflammation, or other shoulder abnormalities. Ultrasound is particularly useful because it can identify tendon changes and guide targeted treatments
In some cases, ultrasound may reveal specific patterns within the tendon tissue that can help physicians identify SIRVA and determine whether the painful tissue is contributing to symptoms. Ultrasound can also be used to guide diagnostic injections or minimally invasive treatments.
While typical vaccine soreness resolves within a few days, SIRVA symptoms may last weeks or months without treatment. Studies have shown that a large percentage of patients experience pain lasting more than one month.
You should consider seeing a physician if:
Pain begins within 48 hours of vaccination
The shoulder becomes difficult to move or lift
Pain persists longer than one week
Symptoms interfere with sleep or daily activities
Prompt evaluation can help determine whether the pain is typical post-vaccination soreness or a condition such as SIRVA.
No. Vaccines remain very safe and effective. Most people only experience mild, temporary soreness at the injection site. SIRVA is rare and usually related to the injection technique rather than the vaccine itself.
de Lusignan S, Damaso S, Ferreira F, et al. Brand-specific enhanced safety surveillance of GSK’s Fluarix Tetra seasonal influenza vaccine in England: 2017/2018 season. Hum Vaccin Immunother. 2020;16:1762–1771.
National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Committee to Review Relevant Literature Regarding Adverse Events Associated with Vaccines. Shoulder Injuries and Vaccine. In: Rosenberg D, Kumova OK, Stratton K, et al, eds. Evidence Review of the Adverse Effects of COVID-19 Vaccination and Intramuscular Vaccine Administration. Washington, DC: National Academies Press (US); 2024.
Sussman WI, Davitt K, Mitchell K, Sussman J, Latzka E. Sonographic Features of Shoulder Injury Related to Vaccine Administration: A Case Series. Clin J Sport Med. 2026 Feb 4. doi:10.1097/JSM.0000000000001415. Epub ahead of print. PMID: 41634920.
Learn how ultrasound-guided percutaneous fasciotomy may revolutionize treatment for chronic exertional compartment syndrome with faster recovery and smaller incisions.
Read MoreResearchers used artificial intelligence and natural language processing to identify Shoulder Injury Related to Vaccine Administration (SIRVA) cases from over 3.7 million vaccinations. Learn what the study found, how
Read More