Email: info@BSBortho.com
Patellar tendinitis, often referred to as jumper’s knee, is one of the most common overuse injuries seen in sports medicine. It affects athletes who perform repetitive jumping, sprinting, or explosive lower body movements, including basketball, volleyball, and track athletes. However, it’s not limited to elite athletes, weekend warriors and active individuals are also at risk. Learn more about patellar tendinitis here.
If you’ve been dealing with persistent pain just below your kneecap that won’t go away despite rest or physical therapy, you may be dealing with patellar tendinopathy, a more chronic and degenerative form of tendon injury. Understanding the condition, and newer minimally invasive treatments like ultrasound-guided tendon scraping, can help guide better recovery.
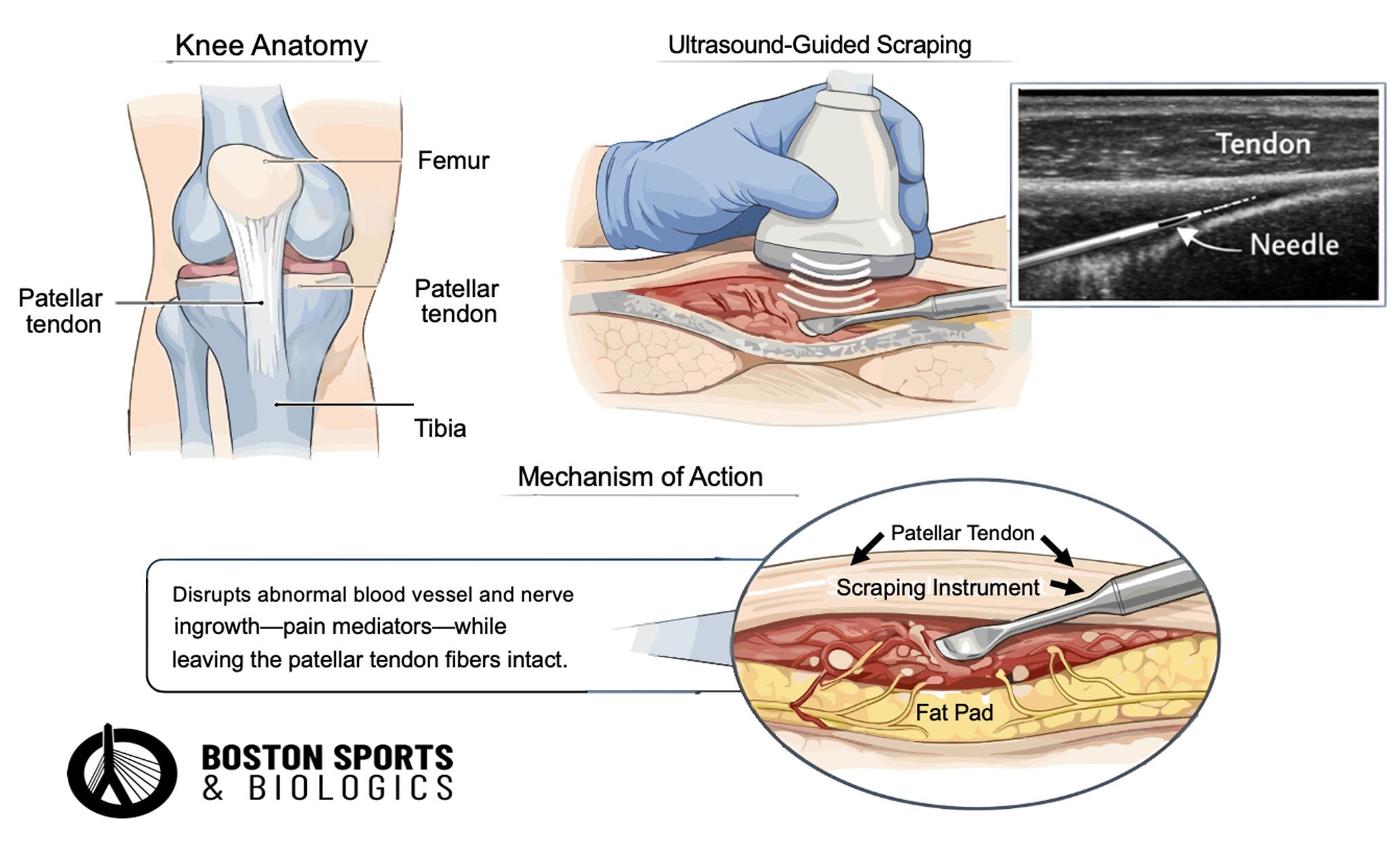
Patellar tendinitis involves irritation or degeneration of the patellar tendon, which connects the kneecap (patella) to the shinbone (tibia). This tendon plays a critical role in knee extension, making it essential for walking, running, and jumping.
The term "tendinitis" is a misnomer, histology consistently shows degeneration, cell death, and micro-tear (Fu et al, 2002). A systematic review of surgical specimens across multiple tendon sites
found that 100% of studies identified at least one element of mucoid degeneration, while only 20% reported any inflammation (Bruni et al, 2023).
While the term “tendinitis” suggests inflammation, most chronic cases actually represent tendinosis, a degenerative process involving:
These changes contribute to persistent pain and reduced function.
The hallmark features are pain localized to the inferior pole of the patella and load-related pain that increases with demand on the knee extensors, particularly in activities that store and release energy in the patellar tendon (Malliaras et al, 2015). Pain at the front of the knee with tenderness to palpation over the tendon are the typical presenting symptoms (Lopes et al, 2025).
Squatting, stair climbing, and prolonged sitting are classic triggers for anterior knee pain in patellar tendinopathy. The condition commonly affects individuals participating in activities requiring repetitive jumping, braking, kicking, or running (Lopes et al, 2025). Patients with patellar tendinopathy typically report:
The characteristic warm-up phenomenon is well-documented in the Blazina classification system, which describes the clinical progression of the disease. Phase 1 presents as pain after exercise only, while Phase 2 is characterized by pain present at the beginning and end of activity but notably absent after warm-up. Phase 3 represents more advanced disease with pain during and after activity (Dan et al, 2019). This progression reflects the degenerative nature of the condition, which typically involves gradually increasing pain in the patellar tendon (Theodorou et al, 2023).
In more advanced cases, even daily activities like stairs or prolonged sitting can become painful.
One of the key drivers of chronic tendon pain is the development of neovascularization, abnormal blood vessel growth into the tendon. These vessels are often accompanied by pain-sensitive nerve fibers, which may contribute significantly to symptoms.
The relationship between neovascularization and pain is complex and bidirectiona (Palee et al, 2025). A 2025 scoping review found that 73% of studies identified neoinnervation (nerve ingrowth) in chronic tendinopathy, with 76.9% highlighting the role of the paratenon as a key site where abnormal blood vessels are accompanied by pain-sensitive nerve fibers.
However, neovascularization plays an ambiguous role—it is crucial for tendon healing but also contributes to degeneration when regeneration is incomplete. The neovascularization process should be reconsidered in tendinopathy scoring systems due to discrepancies in studies, as it can represent both a healing response and a pathological feature (Jaworski et al, 2022).
This helps explain why:
The dissociation between imaging findings and pain is well-documented. A 2026 study of 76 athletes found no significant associations between baseline imaging abnormalities (including Doppler flow, tendon thickness, fiber disruption, or bone marrow edema) and 24-week changes in pain or disability scores, leading authors to conclude that "healthcare professionals should avoid relying on conventional imaging findings to predict prognosis." This occurs because structural changes on imaging do not directly correlate with symptom severity—some athletes have significant structural abnormalities without pain, while others have severe pain with minimal imaging changes (Zhang et al, 2014; Deng et al, 2026).
Most patients improve with non-surgical care, including:
Strong evidence supports exercise-based rehab as a cornerstone of treatment. A 2025 Cochrane systematic review found moderate-certainty evidence that exercise improves pain and function compared to no treatment, with improvements maintained at 12 months (Lopes et al, 2025).
These aim to modulate healing or target neovascularity. However, some patients fail to improve—especially those with long-standing symptoms.
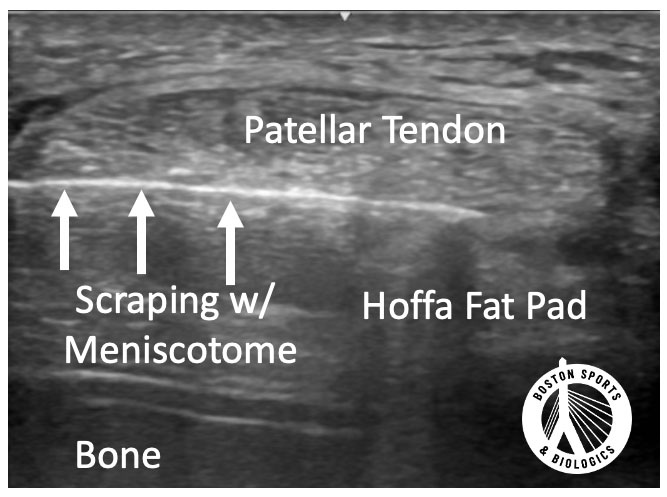
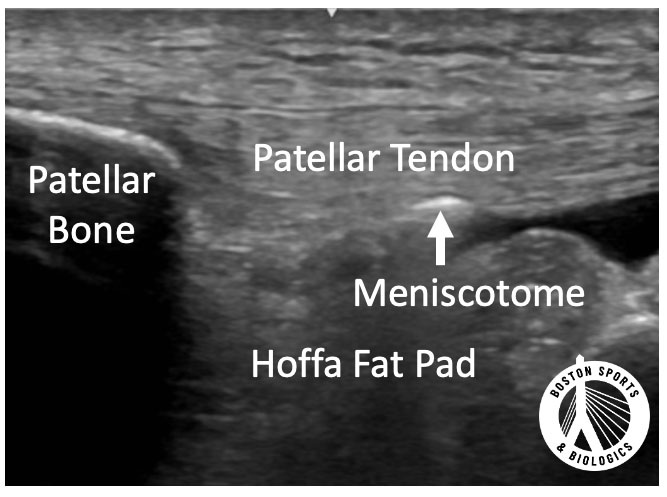
Ultrasound-guided tendon scraping is a minimally invasive procedure designed to target the pain-generating interface between the tendon and surrounding tissue, without damaging the tendon itself.
The procedure targets the pain-generating interface between the tendon and surrounding tissue. There has been recent interest regarding the neurogenic influences involved in chronic tendinopathy, and interventions targeting neovessels and accompanying neonerves have shown promise (Hall & Rajasekaran, 2016; Baria et al, 2020).
The procedure is performed:
Importantly, the tendon itself is not cut or weakened, making this a low-risk approach. The goal of tendon scraping is to:
The concept of tendon scraping is rooted in the pioneering work of Håkan Alfredson in the treatment of chronic Achilles tendinopathy and has since been adapted for use in other tendons, including the patellar tendon (Alfredson, 2011). The procedure is performed under local anesthesia using ultrasound guidance. A small skin entry point is created, and a needle is advanced to the space between the tendon and the adjacent fat pad. Importantly, the technique remains extra-tendinous. The needle is then used to mechanically separate the tendon from the surrounding soft tissue, disrupting abnormal blood vessel and nerve ingrowth thought to contribute to pain. In Alfredson’s early experience treating noninsertional Achilles tendinopathy, most patients demonstrated meaningful pain reduction in 74% of patients.
Application of this technique to the patellar tendon is more limited in the literature. A published case report by Hall and Rajasekaran described a competitive athlete who experienced rapid symptom improvement within two weeks, returned to sport by four weeks, and was able to complete the season without requiring additional intervention (Hall & Rajasekaran, 2016).
More recently, Baria and colleagues expanded on this concept in a small case series evaluating ultrasound-guided patellar tendon scraping. Their findings demonstrated clinically meaningful improvement in the majority of patients, with high rates of return to sport and no major complications, supporting the procedure as a safe, minimally invasive option for managing recalcitrant patellar tendinopathy (Baria et al, 2020).
Although still emerging, Baria et al showed:
Compared to traditional surgical options, tendon scraping is a
minimally invasive, office-based procedure, does not disruption the
tendon structure, and provides a recovery timeline often in weeks.
Patients are often able to:
Importantly, because the procedure is extra-tendinous, the risk of tendon rupture is very low compared to some other interventions .
“Tendinitis” implies inflammation, while tendinosis refers to chronic degeneration of the tendon. Most long-standing cases are actually tendinosis.
With proper rehab, mild cases may improve in 6–12 weeks. Chronic cases can take several months, and sometimes require advanced treatments.
Tendon scraping is less invasive, has faster recovery, and preserves tendon integrity. It may be a good alternative before considering surgery.
Yes. In early studies, athletes returned to sport in as little as 3–4 weeks, depending on symptoms and progression .
PRP can be effective for some patients, but results vary. It may be used alone or in combination with other treatments.
The procedure is done under local anesthesia. Most patients tolerate it well and report only mild post-procedure soreness.
A sports medicine physician with expertise in musculoskeletal ultrasound and minimally invasive procedures is best equipped to evaluate and treat this condition.
Alfredson H. Ultrasound and Doppler-guided mini-surgery to treat midportion Achilles tendinosis: results of a large material and a randomised study comparing two scraping techniques. Br J Sports Med. 2011 Apr;45(5):407-10. doi: 10.1136/bjsm.2010.081216. Epub 2011 Feb 23. PMID: 21349878.
Baria, Michael & Plunkett, Evan & Miller, Meghan & Borchers, James & Miller, Timothy & Magnussen, Robert. Ultrasound-guided Percutaneous Tendon Scraping: A Novel Technique for Treating Patellar Tendinopathy. Techniques in Orthopaedics. Publish Ahead of Print. (2020).;1. doi: 10.1097/BTO.0000000000000471.
Bruni DF, Pierson SR, Sarwar F, Ring D, Ramtin S. Are the Pathologic Features of Enthesopathy, Tendinopathy, and Labral and Articular Disc Disease Related to Mucoid Degeneration? A Systematic Review. Clin Orthop
Relat Res. 2023 Apr 1;481(4):641-650. doi: 10.1097/CORR.0000000000002499. Epub 2022 Dec 23. PMID: 36563131; PMCID: PMC10013668.
Dan M, Phillips A, Johnston RV, Harris IA. Surgery for patellar tendinopathy (jumper's knee). Cochrane Database Syst Rev. 2019 Sep 23;9(9):CD013034. doi: 10.1002/14651858.CD013034.pub2. PMID: 31546279; PMCID: PMC6756823.
Deng J, Breda SJ, Fang Y, Eygendaal D, de Vos RJ, Oei EHG. Prognostic Value of Conventional Ultrasound and MRI Features for Clinical Outcomes in Athletes With Patellar Tendinopathy After Exercise Therapy. Sports Health. 2026 Jan 26:19417381251401164. doi: 10.1177/19417381251401164. Epub ahead of print. PMID: 41588720; PMCID: PMC12846899.
Fu SC, Wang W, Pau HM, Wong YP, Chan KM, Rolf CG. Increased expression of transforming growth factor-beta1 in patellar tendinosis. Clin Orthop Relat Res. 2002 Jul;(400):174-83. doi: 10.1097/00003086-200207000-00022. PMID: 12072760.
Hall MM, Rajasekaran S. Ultrasound-Guided Scraping for Chronic Patellar Tendinopathy: A Case Presentation. PM R. 2016 Jun;8(6):593-6. doi: 10.1016/j.pmrj.2015.10.013. Epub 2015 Nov 6. PMID: 26548965.
Jaworski Ł, Zabrzyńska M, Klimaszewska-Wiśniewska A, Zielińska W, Grzanka D, Gagat M. Advances in Microscopic Studies of Tendinopathy: Literature Review and Current Trends, with Special Reference to Neovascularization Process. J Clin Med. 2022 Mar 13;11(6):1572. doi: 10.3390/jcm11061572. PMID: 35329898; PMCID: PMC8949578.
Lopes AD, Rizzo RR, Hespanhol L, Costa LO, Kamper SJ. Exercise for patellar tendinopathy. Cochrane Database Syst Rev. 2025 May 27;5(5):CD013078. doi: 10.1002/14651858.CD013078.pub2. PMID: 40421598; PMCID: PMC12107522.
Malliaras P, Cook J, Purdam C, Rio E. Patellar Tendinopathy: Clinical Diagnosis, Load Management, and Advice for Challenging Case Presentations. J Orthop Sports Phys Ther. 2015 Nov;45(11):887-98. doi: 10.2519/jospt.2015.5987. Epub 2015 Sep 21. PMID: 26390269.
Palee S, Jarusriwanna A, Lee D, Yener U, Kaye AD, Shaparin N, Wahezi SE. Chronic Tendinopathy Driven by Neoinnervation: The Role of the Paratenon, Upregulated Neural Biomarkers, and Evolving Evidence - A Scoping Review. Pain Physician. 2025 Jul;28(4):287-297. PMID: 40773634.
Theodorou A, Komnos G, Hantes M. Patellar tendinopathy: an overview of prevalence, risk factors, screening, diagnosis, treatment and prevention. Arch Orthop Trauma Surg. 2023 Nov;143(11):6695-6705. doi: 10.1007/s00402-023-04998-5. Epub 2023 Aug 4. PMID: 37542006; PMCID: PMC10541843.
Zhang ZJ, Ng GY, Lee WC, Fu SN. Changes in morphological and elastic properties of patellar tendon in athletes with unilateral patellar tendinopathy and their relationships with pain and functional disability. PLoS One. 2014 Oct 10;9(10):e108337. doi: 10.1371/journal.pone.0108337. PMID: 25303466; PMCID: PMC4193737.
Learn how ultrasound-guided percutaneous fasciotomy may revolutionize treatment for chronic exertional compartment syndrome with faster recovery and smaller incisions.
Read MoreResearchers used artificial intelligence and natural language processing to identify Shoulder Injury Related to Vaccine Administration (SIRVA) cases from over 3.7 million vaccinations. Learn what the study found, how
Read More