Email: info@BSBortho.com
Patellar tendinopathy is a common overuse injury affecting the patellar tendon, which connects the knee cap to the shin bone, and helps straighten the knee. Stress is greatest across the patellar tendon when jumping and landing, and patellar tendinopathy or tendinosis is often seen in athletes involved in sports that require repetitive jumping and running, such as basketball and volleyball.
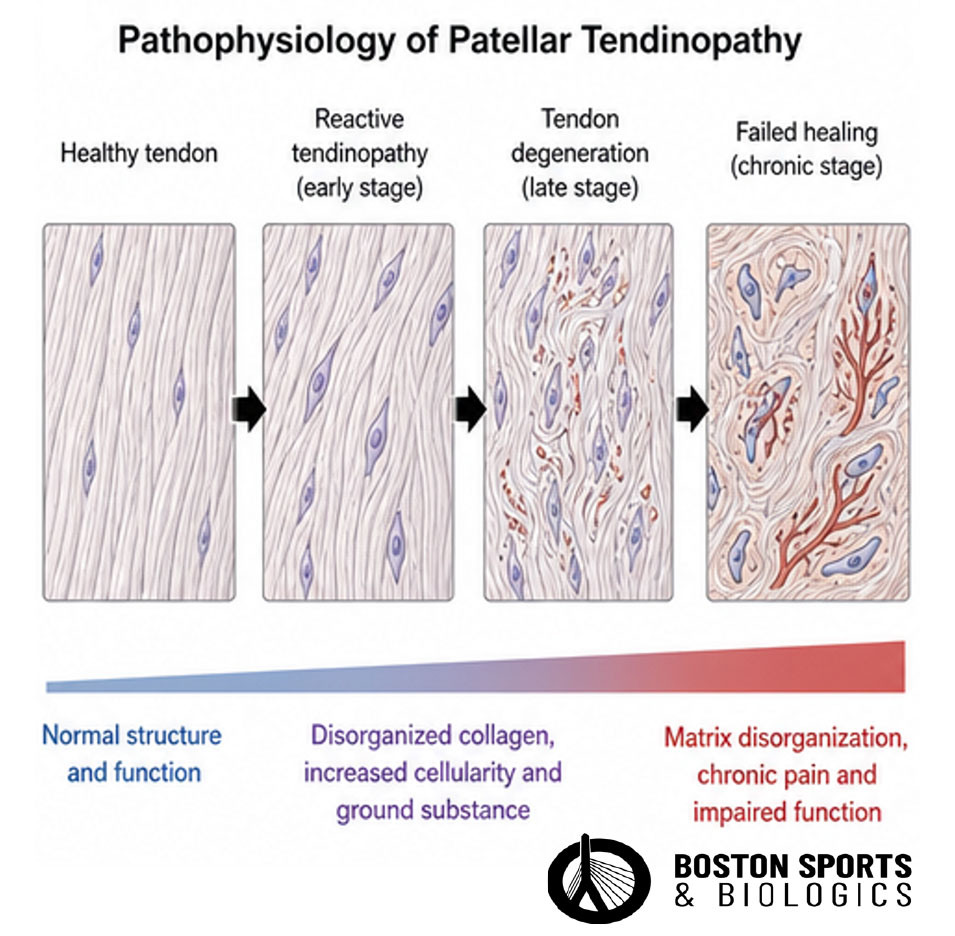
Patellar tendinosis, also often referred to as “jumper’s knee,” involves a degenerative process rather than an inflammatory one. Patellar tendinosis is marked by microinjury to the tendon fibers, leading
to mucoid degeneration, necrosis, and loss of transitional fibrocartilage [Figueroa et al, 2016; Arner et al, 2024].
Histologically, the tendon develops a disrupted abnormal collagen matrix, increased cellularity, and increased proteoglycan content without significant inflammatory cell infiltration [Fu et al, 2002].
The patellar tendon is part of the knee's extensor mechanism. The tendons primary function is transmitting force from the quadriceps muscle to extend the knee during activities such as running, jumping, and climbing stairs.
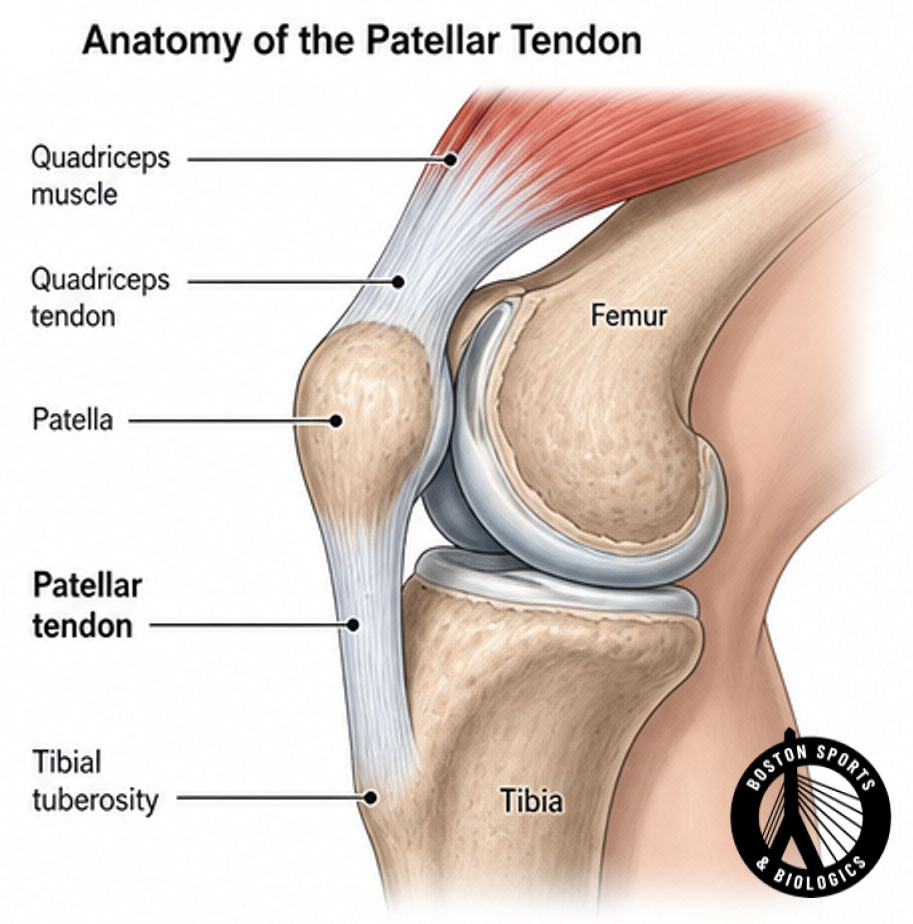
The most common location of injury is the proximal patellar tendon, where the tendon attaches to the inferior pole of the patella. Repetitive loading can result in collagen disorganization, tendon thickening, neovascularization, and degenerative changes within the tendon.
The clinical symptoms of patellar tendinopathy, also known as patellar tendinosis, include:
Localized Pain: Pain is typically localized to the inferior pole of the patella. This pain is often described as sharp or aching and is exacerbated by activities that load the knee extensors, such as jumping, running, or squatting [Malliaras et al, 2015; Fredberg & Bolvig, 1999]. Distal patellar tendinopathy can present with pain over the tibial tubercle.
Activity-Related Pain: The pain typically increases with activities that involve repetitive knee extension and high-impact loading, such as sports involving jumping and running [Malliaras et al, 2015; Rosen et al, 2022].
Tenderness on Palpation: There is tenderness to palpation of the patellar tendon, particularly at its attachment to the inferior pole of the patella [Fredberg & Bolvig, 1999; Garau et al, 2008].
Swelling: Some patients may experience localized swelling around the patellar tendon, although this is not always present [Fu et al, 2002].
Functional Impairment: Patients often report diminished flexibility, reduced strength, and decreased physical function, which can impact their ability to perform athletic activities [Rosen et al, 2022].
Conservative Management
Nonsurgical options historically included rest, ice, medication and physical therapy. Imaging, including an MRI or musculoskeletal ultrasound, will often confirm the diagnosis [Arner et al, 2024; Everhart et al, 2017; Vander Doelen & Jelley, 2020; Larsson et al, 2012].
Corticosteroid injections are generally not recommended due to their lack of long-term benefit and potential for tendon rupture [Everhart et al, 2017; Irby et al, 2020].
Extracorporeal shock wave therapy (ESWT):
Extracorporeal shock wave therapy has shown moderate effectiveness in some studies [Everhart et al, 2017; Larsson et al, 2012; Irby et al, 2020].
Platelet-rich plasma (PRP) injections:
Platelet-rich plasma (PRP) injections have shown promise in the available studies, particularly with multiple injections, for long-term improvement [Vander Doelen & Jelley, 2020; Andriolo et al, 2019; Chen et al, 2019].
Dry needling:
This can be effective for pain reduction and functional improvement [Vander Doelen & Jelley, 2020].
Surgical intervention
Surgical intervention is considered for patients who do not respond to conservative treatments after 6 months. Options include:
Open or arthroscopic debridement: Both methods have shown similar outcomes, though no high-quality comparison studies exist [Arner et al, 2024; Everhart et al, 2017; Figueroa et al, 2016].
Suture anchor repair: Used when necessary during open procedures [Arner et al, 2024].
References
Andriolo L, Altamura SA, Reale D, Candrian C, Zaffagnini S, Filardo G. Nonsurgical Treatments of Patellar Tendinopathy: Multiple Injections of Platelet-Rich Plasma Are a Suitable Option: A Systematic Review and Meta-analysis. Am J Sports Med. 2019 Mar;47(4):1001-1018.
Arner JW, Kaeding CC, Bradley JP. Management of Patellar Tendinopathy. Arthroscopy. 2024 Jan;40(1):13-15.
Chen PC, Wu KT, Chou WY, Huang YC, Wang LY, Yang TH, Siu KK, Tu YK. Comparative Effectiveness of Different Nonsurgical Treatments for Patellar Tendinopathy: A Systematic Review and Network Meta-analysis. Arthroscopy. 2019 Nov;35(11):3117-3131.e2.
Everhart JS, Cole D, Sojka JH, Higgins JD, Magnussen RA, Schmitt LC, Flanigan DC. Treatment Options for Patellar Tendinopathy: A Systematic Review. Arthroscopy. 2017 Apr;33(4):861-872.
Figueroa D, Figueroa F, Calvo R. Patellar Tendinopathy: Diagnosis and Treatment. J Am Acad Orthop Surg. 2016 Dec;24(12):e184-e192.
Fredberg U, Bolvig L. Jumper's knee. Review of the literature. Scand J Med Sci Sports. 1999 Apr;9(2):66-73.
Fu SC, Wang W, Pau HM, Wong YP, Chan KM, Rolf CG. Increased expression of transforming growth factor-beta1 in patellar tendinosis. Clin Orthop Relat Res. 2002 Jul;(400):174-83.
Garau G, Rittweger J, Mallarias P, Longo UG, Maffulli N. Traumatic patellar tendinopathy. Disabil Rehabil. 2008;30(20-22):1616-20.
Irby A, Gutierrez J, Chamberlin C, Thomas SJ, Rosen AB. Clinical management of tendinopathy: A systematic review of systematic reviews evaluating the effectiveness of tendinopathy treatments. Scand J Med Sci Sports. 2020 Oct;30(10):1810-1826.
Larsson ME, Käll I, Nilsson-Helander K. Treatment of patellar tendinopathy--a systematic review of randomized controlled trials. Knee Surg Sports Traumatol Arthrosc. 2012 Aug;20(8):1632-46.
Malliaras P, Cook J, Purdam C, Rio E. Patellar Tendinopathy: Clinical Diagnosis, Load Management, and Advice for Challenging Case Presentations. J Orthop Sports Phys Ther. 2015 Nov;45(11):887-98.
Nishida Y, Nishino T, Tanaka K, Onishi S, Kanamori A, Yamazaki M. An Objective Measure of Patellar Tendon Thickness Based on Ultrasonography and MRI in University Athletes. J Clin Med. 2021 Sep 10;10(18):4092.
Ostlere S. The extensor mechanism of the knee. Radiol Clin North Am. 2013 May;51(3):393-411.
Rosen AB, Wellsandt E, Nicola M, Tao MA. Clinical Management of Patellar Tendinopathy. J Athl Train. 2022 Jul 1;57(7):621-631.
Tyler TF, Hershman EB, Nicholas SJ, Berg JH, McHugh MP. Evidence of abnormal anteroposterior patellar tilt in patients with patellar tendinitis with use of a new radiographic measurement. Am J Sports Med. 2002 May-Jun;30(3):396-401.
Vander Doelen T, Jelley W. Non-surgical treatment of patellar tendinopathy: A systematic review of randomized controlled trials. J Sci Med Sport. 2020 Feb;23(2):118-124.
Warden SJ, Kiss ZS, Malara FA, Ooi AB, Cook JL, Crossley KM. Comparative accuracy of magnetic resonance imaging and ultrasonography in confirming clinically diagnosed patellar tendinopathy. Am J Sports Med. 2007 Mar;35(3):427-36.