Email: info@BSBortho.com
What is Knee Arthritis?
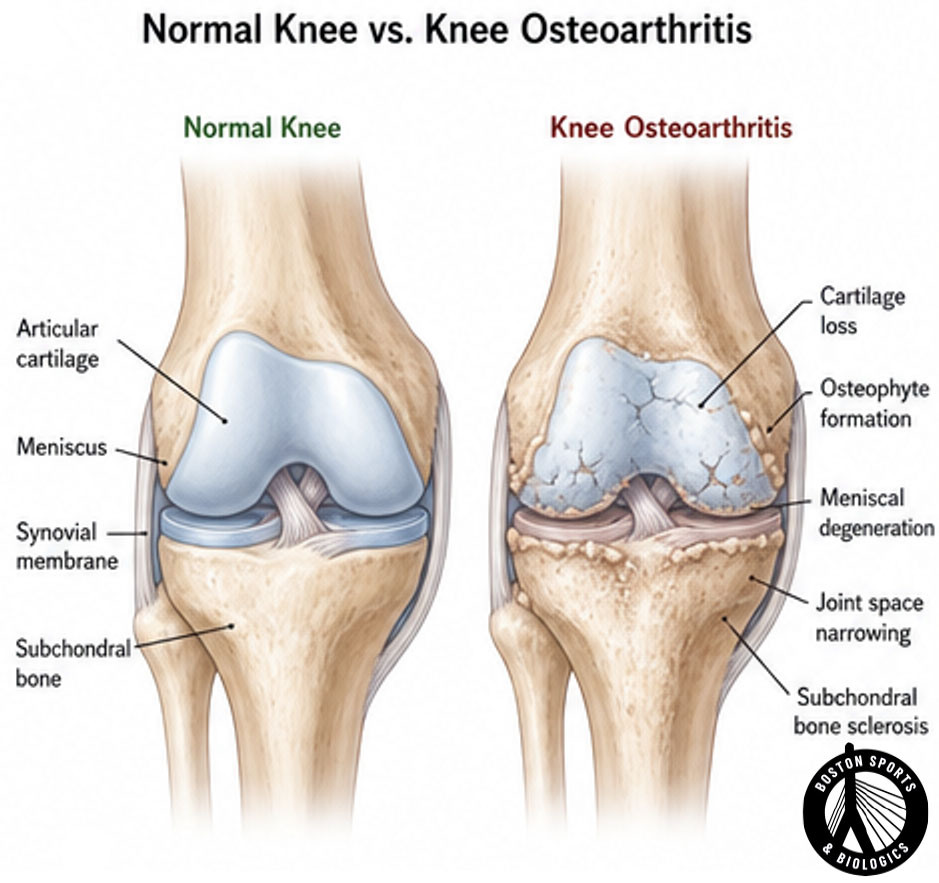
The knee is the largest joint in the body and consists of three compartments:
Healthy cartilage covers the ends of the femur, tibia, and patella, allowing smooth movement with minimal friction. The menisci act as shock absorbers and help distribute load across the joint.
As osteoarthritis progresses, cartilage becomes thinner, the menisci may degenerate, bone spurs (osteophytes) can develop, and inflammation within the joint increases.
The diagnosis of knee OA is primarily clinical, based on history and physical examination. Patients often report knee pain, inflammation and stiffness.
Symptoms often develop gradually over time. Symptoms may fluctuate and often worsen with increased activity. Common symptoms include:
On examination, patients can have joint line tenderness, bony enlargement, and restricted movement [Katz et al, 2021; Duong et al, 2023; Ebell, 2018]. Common findings include:
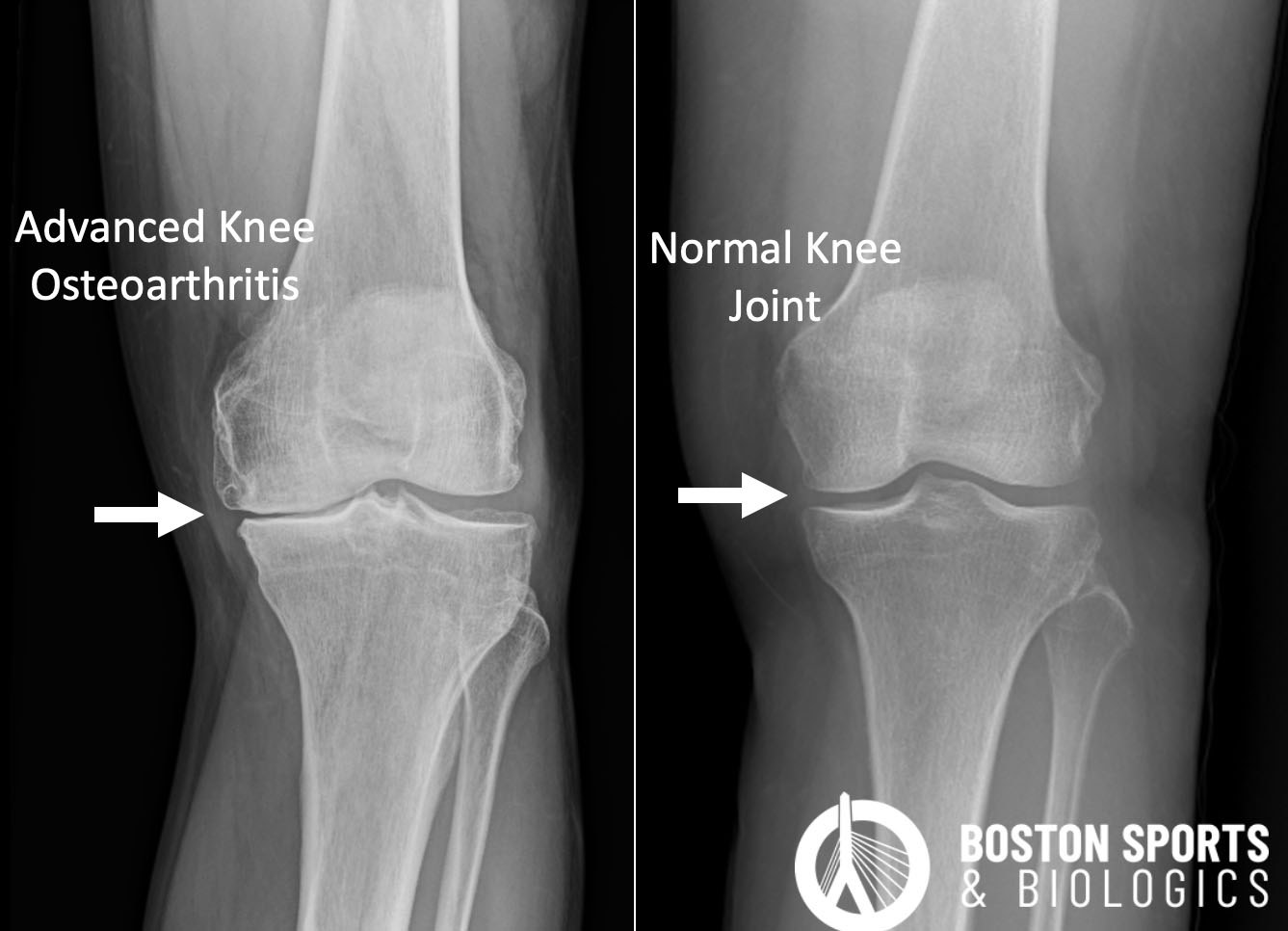
Radiographs
may be needed to confirm the diagnosis. Weight-bearing x-rays can show
joint space narrowing, spurs (osteophytes), bone thickening (subchondral
sclerosis), and cysts.
MRI is not routinely required but can be useful in complex cases [Katz et al, 2021; Duong et al, 2023; Ebell, 2018].
Nonsurgical options historically included:
Many patients are not ready for a joint replacement and there are a number of strategies to help manage pain until you are ready or the disease is severe enough to warrant surgery. The goal of treatment is to control the pain. Various evidence supports medications, weight loss, bracing, physical therapy, and cortisone injections.
Corticosteroid injections:
Intra-articular corticosteroid injections have been shown to provide short-term pain relief and are recommended for acute exacerbations of knee OA. They are effective in reducing pain and improving function, but their benefits are typically short-lived [Beaudart et al, 2020; Bannuru et al, 2015; Brophy & Fillingham, 2022; Kolasinski et al, 2020].
Viscosupplementation injections:
Viscosupplementation injections, or intra-articular hyaluronic acid injections, are commonly used for knee pain, and have been approved by the US Food and Drug Administration (FDA) since 1997 [Beaudart et al, 2020; Bannuru et al, 2015; Brophy & Fillingham, 2022].
Learn more about viscosupplementation injections for knee pain here.
Orthobiologic Injections:
What is the evidence for platelet-rich plasma (PRP) in the treatment of knee osteoarthritis (OA)?
Platelet-rich plasma (PRP) has been studied for knee osteoarthritis (OA) and can be effective in temporarily reducing pain and improving function, with recent studies highlighting the importance of platelet dose:
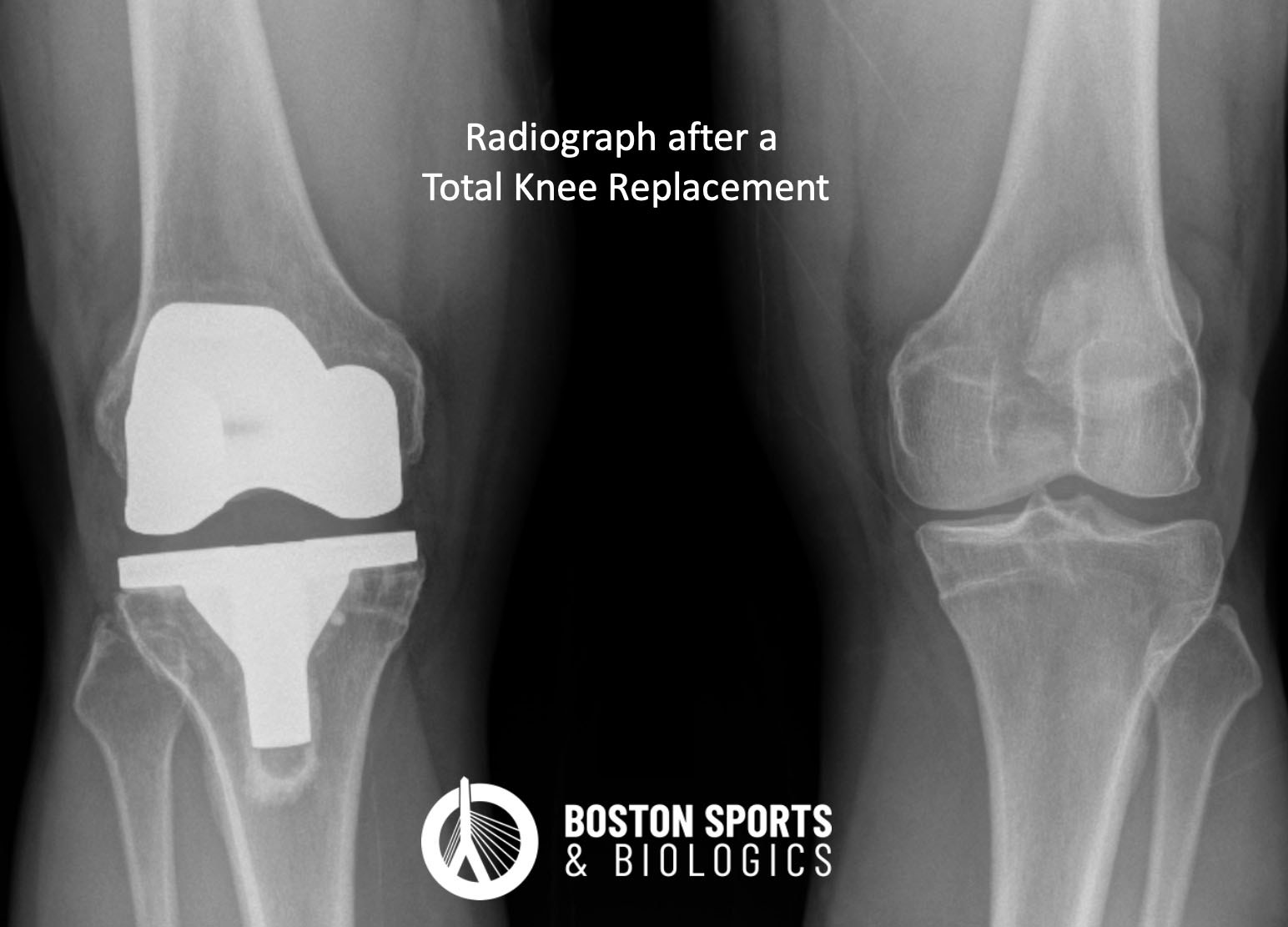
Surgical Management
What are the long-term outcomes of platelet-rich plasma (PRP) treatment for knee osteoarthritis?
The long-term outcomes of platelet-rich plasma (PRP) treatment for knee osteoarthritis (OA) are influenced by the platelet dose and the number of injections.
What is the role of higher platelet doses for the treatment of knee osteoarthritis?
What is the role of multiple injections for the treatment of knee osteoarthritis?
What is long-term efficacy of PRP for the treatment of knee osteoarthritis?
There is no single best treatment. Management typically combines exercise, physical therapy, weight management, and targeted interventions based on symptom severity.
Many studies demonstrate that PRP provides longer-lasting improvements than corticosteroid injections for knee osteoarthritis.
Current evidence suggests PRP may improve symptoms and joint health, but complete cartilage regeneration has not been consistently demonstrated.
Most orthobiologic procedures are considered elective and are not currently covered by insurance.
Joint replacement is generally considered when symptoms significantly impair quality of life and conservative treatment options no longer provide adequate relief.
Maintaining a healthy weight, staying active, addressing injuries promptly, and optimizing joint mechanics may reduce the risk of osteoarthritis progression.
References:
(781) 591-7855
20 Walnut St
Suite 14
Wellesley MA 02481