Email: info@BSBortho.com
Chronic Exertional Compartment Syndrome (CECS) is a common cause of exercise-induced leg pain in runners, athletes, military personnel, and active individuals. The condition occurs when pressure builds within one or more muscle compartments during activity, leading to reduced blood flow, nerve irritation, and pain.
Unlike acute compartment syndrome, CECS is not a medical emergency. Symptoms typically develop predictably during exercise and improve with rest. However, the condition can significantly limit athletic performance and quality of life if left untreated.
At Boston Sports & Biologics, we specialize in the diagnosis of CECS using dynamic compartment pressure testing and offer minimally invasive ultrasound-guided compartment release procedures as an alternative to traditional open surgery.
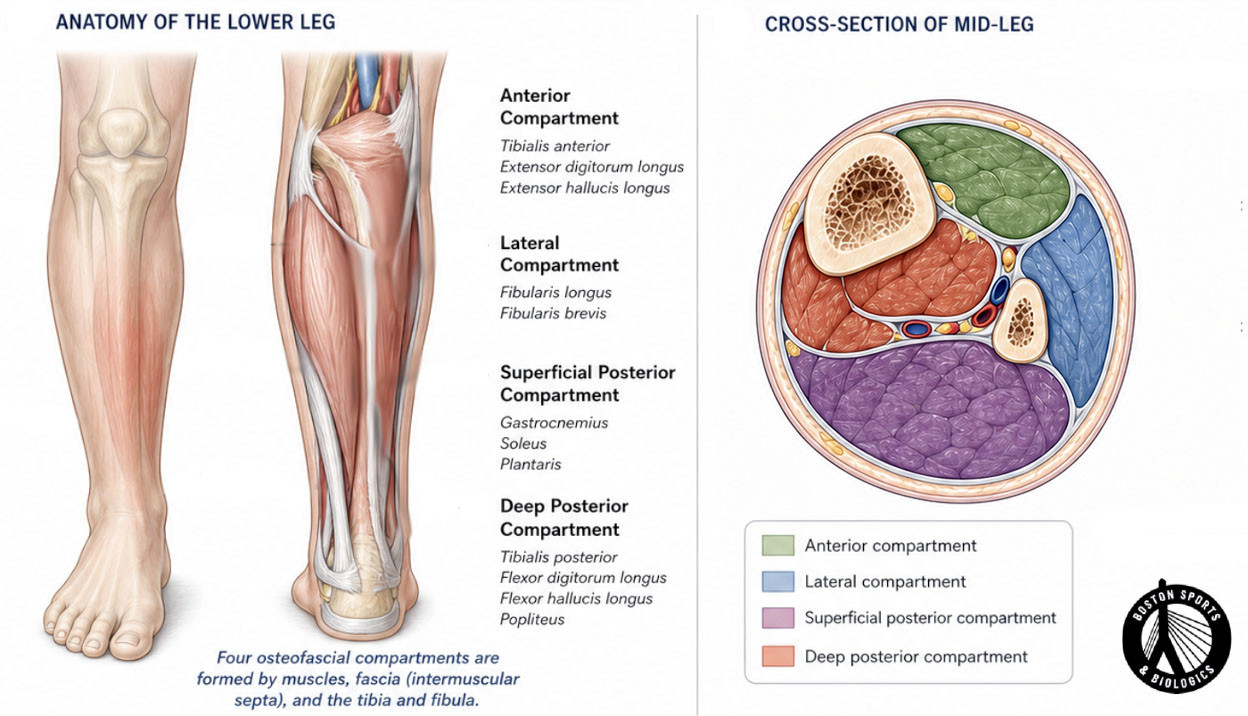
The muscles of the lower leg are organized into separate compartments surrounded by strong connective tissue called fascia. During exercise, muscles naturally expand as blood flow increases.

In patients with CECS, the fascia may not expand sufficiently, causing pressure to build within the compartment. As pressure rises, blood flow becomes restricted, and nerves may become compressed, producing pain and other symptoms.
The condition most commonly affects the:
The anterior and lateral compartments are involved in more than 90% of cases.
The hallmark feature of CECS is pain that occurs at a predictable point during exercise and improves with rest.
Common symptoms include:
Many patients describe feeling normal at rest but developing symptoms every time they run, hike, cycle, or participate in sports.
CECS most commonly affects:
The condition is most frequently seen in young, active individuals but can occur at any age.
Several other conditions can cause exercise-related leg pain, including:
Because many of these conditions produce similar symptoms, a thorough evaluation is critical.
Diagnosis begins with a detailed history and physical examination.
Several features strongly suggest CECS:
The current gold standard for diagnosis is dynamic intracompartmental pressure testing.
During this procedure:
Elevated compartment pressures support the diagnosis of CECS and help determine which compartments are involved.
Diagnostic musculoskeletal ultrasound may also be used to:
Non-surgical treatment may be attempted initially and can include:
Reducing or temporarily avoiding symptom-provoking activities may help control symptoms.
Treatment may focus on:
Recent research suggests that transitioning from a heel-strike pattern toward a forefoot or midfoot strike may reduce compartment pressures in some runners.
Changes in training volume, terrain, footwear, and running mechanics may provide symptom relief in selected patients.
Botulinum toxin injections have been investigated as a potential treatment for CECS, although long-term evidence remains limited.
Unfortunately, many athletes with persistent CECS symptoms ultimately require surgical treatment to return to their desired activity level.
Traditional treatment for CECS involves open fasciotomy, which requires surgical incisions to release the constricting fascia.
Boston Sports & Biologics offers minimally invasive ultrasound-guided compartment release in appropriately selected patients.
Compared with traditional open surgery, ultrasound-guided procedures may offer:
Using ultrasound guidance, the fascia can be precisely released through small incisions while protecting surrounding structures.
Boston Sports & Biologics specializes in:
Our goal is to accurately identify the source of your symptoms and develop a treatment plan that helps you return to the activities you enjoy.
If you experience predictable leg pain, tightness, numbness, or weakness during exercise, chronic exertional compartment syndrome may be the cause.
Contact Boston Sports & Biologics to schedule a comprehensive evaluation and determine whether compartment pressure testing or minimally invasive ultrasound-guided treatment may be appropriate for you.
(781) 591-7855
20 Walnut St
Suite 14
Wellesley MA 02481
Unlike acute compartment syndrome, CECS is not typically limb-threatening. However, it can significantly limit exercise and athletic performance.
Some patients improve with activity modification or gait retraining, but many athletes experience persistent symptoms without treatment.
Not always. Conservative treatment is often attempted first. Surgical intervention is generally considered when symptoms persist despite non-operative care.
Most studies report favorable outcomes following fasciotomy, with many patients returning to sports and physical activity.
For appropriately selected patients, ultrasound-guided release may provide a minimally invasive alternative to traditional open fasciotomy.