Email: info@BSBortho.com
Patients suffering from arthritis, tendon injuries, back pain, and sports-related conditions are increasingly exposed to advertisements for "stem cell injections" derived from amniotic fluid, amniotic membrane, umbilical cord tissue, and Wharton's jelly. These products are often promoted as cutting-edge regenerative medicine capable of repairing damaged tissues without surgery.
However, the regulatory and scientific reality is far more complex.
In recent years, the U.S. Food and Drug Administration (FDA) has issued multiple warning letters to manufacturers of amniotic and umbilical cord-derived products, stating that many of these products are unapproved biologic drugs.
At the same time, questions remain regarding whether commercially available birth-tissue products contain viable stem cells after processing, cryopreservation, shipping, and storage.
Understanding how these products are manufactured, what they actually contain, and how they differ from laboratory-expanded stem cell therapies is essential for both physicians and patients.
The evidence regarding birth-tissue products in regenerative medicine reveals a significant gap between marketing claims and demonstrated clinical efficacy, with particular concern about the characterization of these products as "stem cell" therapies.
Birth-tissue products are derived from tissues collected following healthy cesarean-section deliveries, including:
• Amniotic fluid
• Amniotic membrane
• Chorion
• Umbilical cord tissue
• Wharton's jelly
• Umbilical cord blood
After donation and screening, these tissues are processed into injectable or implantable products marketed for a variety of orthopedic and regenerative medicine applications.
Many advertisements refer to these products as "stem cell" therapies. However, the actual cellular composition of commercially available products can vary dramatically depending on processing methods, preservation techniques, and storage conditions.
Commercially available perinatal products that have been independently tested contain biologically active molecules but no viable human cells, mesenchymal stem cells (MSCs), or
otherwise (Fortier et al, 2021). Independent laboratory analysis of a cord blood product found that cell viability was lower than manufacturer claims, the cells present were primarily leukocytes, with no stem cells were identified, and growth factor concentrations were falsely elevated due to nonspecific antibody binding in ELISA assays (Fortier et al, 2021).

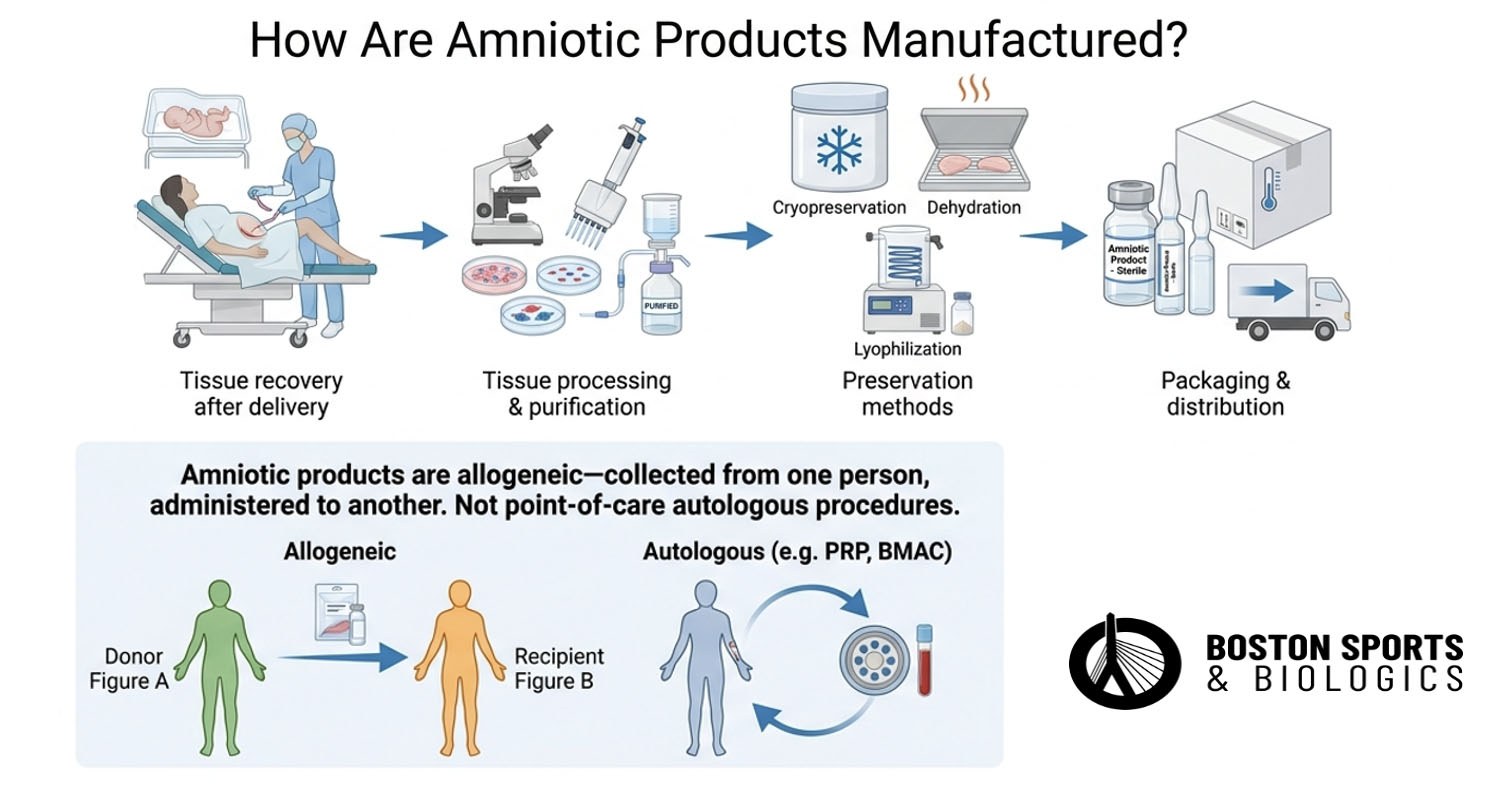
The manufacturing process typically involves several steps:
Unlike autologous procedures such as platelet-rich plasma (PRP) or bone marrow aspirate concentrate (BMAC), these products are collected from one individual and administered to another. This makes them allogeneic biologic products rather than autologous point-of-care procedures.
Many commercially available products undergo extensive processing intended to improve shelf life and allow nationwide distribution.
The FDA regulates human cells, tissues, and cellular and tissue-based products (HCT/Ps) under specific criteria.
To qualify for regulation solely as a tissue product under Section 361 of the Public Health Service Act, a product generally must be:
• Minimally manipulated
• Intended for homologous use
• Not combined with other substances
• Not dependent on living cells for its primary effect
Many birth-tissue products marketed for orthopedic conditions fail to meet these criteria because they are promoted for purposes unrelated to the tissue's original biological function. The FDA has repeatedly stated that products derived from amniotic fluid, Wharton's jelly, and umbilical cord tissue marketed for orthopedic conditions are generally considered biological drugs requiring FDA approval before marketing.
Importantly, the FDA has specifically stated that these products have not been approved for osteoarthritis, tendon injuries, back pain, tennis elbow, or other orthopedic disorders.
One of the most controversial questions surrounding birth-tissue products involves cell viability.
Multiple independent laboratory studies have directly tested commercially available birth-tissue products and found that most do not contain viable mesenchymal stem cells (MSCs).
Many commercial products are marketed as containing mesenchymal stem cells (MSCs). However, multiple studies have demonstrated that preservation methods can significantly affect cell survival.
Cryopreservation, freeze-thaw cycles, transportation, storage, and terminal processing can reduce cellular viability. Several investigators have questioned whether meaningful numbers of viable cells remain in many commercially distributed products by the time they are injected into patients (Moraes et a, 2021; Wolbank et al, 2009).
This does not necessarily mean that the products lack biological activity. Amniotic tissues contain extracellular matrix proteins, cytokines, growth factors, and anti-inflammatory molecules that may persist even when viable cells are absent (Koob et al, 2014).
However, the presence of these molecules is very different from the presence of living, functional stem cells capable of expansion and differentiation, and the American Medical Society for Sports Medicine (AMSSM) position statement explicitly states that currently available perinatal products that have been tested contain biologically active molecules but no viable human cells, MSC, or otherwise (Finnoff et al, 2021).
Cryopreservation is designed to preserve tissue structure and cellular function through ultra-low-temperature storage.
Some studies have demonstrated that carefully controlled cryopreservation methods can preserve viable cells within amniotic membrane tissues and maintain important biologic properties.
However, outcomes vary substantially depending on:
• Tissue type: Moraes et al. found that cryopreservation reduced cell viability differently across anatomical regions, with the placental amnion region showing greater viability loss than the reflected amnion. Dulugiac et al. demonstrated that cells from different umbilical cord compartments (Wharton's jelly, vein, arteries) respond differently to cryopreservation (Dulugiac et al, 2015; Moraes et a, 2021).
• Processing method and cryoprotectant choice: Wagner et
al. showed that glycerol-supplemented cryopreservation yielded higher
cell viability and bFGF secretion than straight freezing at -80°C for up
to 3 months, though differences disappeared by 6 months.
Pogozhykh et al. identified DMSO and propanediol as the most
appropriate cryoprotective agents for placental MSCs, with cooling rate
of 1°C/min to -40°C followed by liquid nitrogen immersion as optimal (Pogozhykh et al, 2015; Wagner et al, 2018).
• Storage duration: The evidence reveals a nuanced picture: structural and extracellular matrix properties tend to be well-preserved over extended periods, but cell viability and functional capacity show time-dependent decline, with the rate of decline varying by tissue type, storage temperature, and cryoprotectant used.
• Freeze-thaw protocols: Whaley et al. confirmed that
cooling and thawing rates have significant influence on cell survival,
with slow cooling (~1°C/min) recommended for MSCs, while rapid cooling
is better for oocytes and embryonic stem cells. Cryoprotectant agents,
while necessary, are themselves toxic at high concentrations and can
cause osmotic stress (Pegg, 2015; Whaley et al, 2021).
• Quality-control procedures: Hennes et al. tested seven
different cryopreservation protocols for amniotic fluid-derived stem
cells and found that three protocols (glycerol-based, generic sperm
freezing medium, and a vitrification method) were unsuccessful due to
low recovery rates and cell viability, while four others performed
well, highlighting the critical importance of protocol selection (Hennes et al. 2015).
More recent publications have highlighted ongoing questions regarding residual cell viability after cryopreservation and whether surviving cells contribute meaningfully to clinical outcomes.
As a result, physicians should be cautious when interpreting claims that commercially available amniotic products contain large numbers of viable stem cells.
One of the biggest misconceptions in regenerative medicine is the assumption that all products marketed as "stem cell therapies" are equivalent. They are not.
Non-Cultured Products
Cultured Stem Cells
Because these expanded-cell products undergo substantial manipulation, the FDA regulates them as biological drugs requiring clinical trials and formal approval.
This distinction is critical. A vial marketed as a "stem cell injection" may bear little resemblance biologically to a laboratory-expanded MSC product used in a clinical trial.
Several countries permit expanded stem-cell therapies under regulatory frameworks that differ substantially from those in the United States. Many of these programs utilize culture-expanded mesenchymal stem cells rather than commercially distributed amniotic products.
Although some international centers have reported promising results, regulatory standards, manufacturing oversight, and clinical evidence vary significantly between jurisdictions. Patients should recognize that availability in another country does not necessarily imply FDA approval or proven effectiveness.
The FDA has significantly increased enforcement efforts against manufacturers of birth tissue, targeted companies producing amniotic fluid, amniotic membrane, umbilical cord, Wharton's jelly, exosome, and related biologic products. FDA warning letters issued in 2024 and 2025 identified numerous products as unapproved drugs and unlicensed biologics.
Many FDA enforcement actions involving regenerative medicine products have involved concerns regarding manufacturing controls, product characterization, and quality assurance. Good Manufacturing Practices (GMP) are quality-control standards used in pharmaceutical and biologic manufacturing.
GMP systems help ensure:
• Product sterility
• Identity
• Purity
• Potency
• Consistency
• Traceability
Without rigorous GMP controls, biologic products may exhibit substantial variability between lots. For cellular therapies, GMP standards become even more important because living cells are highly sensitive to handling, storage, and processing conditions.
One of the major concerns with amniotic, umbilical cord, Wharton’s jelly, and other birth-tissue products is that physicians may rely on manufacturer-supplied safety documents, certificates of analysis, or third-party laboratory reports that do not actually prove the product is FDA-approved, clinically effective, sterile at the time of injection, or legally marketed.
The FDA has repeatedly warned that many regenerative products marketed for arthritis, tendon injuries, chronic pain, and orthopedic conditions are unapproved drugs and biological products. A certificate of analysis may confirm that a specific lot underwent certain tests, but it does not necessarily prove that:
This distinction matters because the physician injecting the product may still be held responsible for what is administered to the patient.
Fraudulent or Misleading Safety Documentation
The risk is not only that documentation may be incomplete. In some regenerative medicine cases, patients and physicians have alleged that safety, sterility, or regulatory representations were misleading or unreliable. A product may be sold with documentation suggesting sterility, donor screening, or quality assurance while still being unlawfully marketed or later associated with contamination.
The Liveyon/Genetech episode is the clearest example. CDC reported bacterial infections after patients received non-FDA-approved umbilical cord blood-derived products processed by Genetech and distributed by Liveyon. Reported infections included bloodstream infections, joint infections, and other serious infections.
A later JAMA Network Open investigation identified 20 patients in eight states with bacterial infections after receiving umbilical cord blood-derived products marketed as stem cell therapies; 19 required hospitalization.
Infection Risk: Why Birth-Tissue Products Are Different
Birth-tissue products are donor-derived biologics. Unlike PRP or BMAC, which are typically autologous point-of-care procedures using the patient’s own tissue, amniotic and umbilical products involve donor recovery, processing, packaging, storage, distribution, and later injection into another person.
Each step introduces potential risks, including donor contamination, inadequate aseptic recovery, processing contamination, incomplete sterility testing, lot-to-lot variability, shipping or storage failures, thawing or handling errors njection into joints, tendons, epidural spaces, or soft tissues
The CDC has emphasized that umbilical cord blood cannot simply be sterilized after collection in the way some non-living products can; therefore, manufacturing controls must prevent contamination from the beginning.
Amniotic fluid, amniotic membrane, Wharton's jelly, and umbilical cord products occupy one of the most controversial areas in regenerative medicine. While these tissues contain biologically active molecules and may possess therapeutic potential, many products marketed as "stem cell injections" differ substantially from true laboratory-expanded stem-cell therapies.
Current FDA policy considers many commercially marketed birth-tissue products to be unapproved biological drugs when promoted for orthopedic conditions. At the same time, questions remain regarding the number of viable cells present after processing and cryopreservation.
Patients considering these treatments should ask important questions:
• Does it contain viable cells?
• What evidence supports its use?
• How was it processed?
• Was it manufactured under GMP standards?
Understanding these distinctions can help patients make informed decisions and avoid marketing claims that may not accurately reflect the underlying science.
No. The FDA has stated that amniotic fluid, Wharton's jelly, and umbilical cord products have not been approved for the treatment of osteoarthritis, tendon injuries, back pain, or other orthopedic conditions.
Some products may contain viable cells depending on processing and preservation methods, but numerous studies have raised concerns regarding cell viability after cryopreservation, storage, and thawing.
Many products are marketed for non-homologous uses and do not meet regulatory criteria for tissue-only regulation, placing them under biologic drug requirements.
No. Most commercially available birth-tissue products are not culture-expanded stem-cell therapies. Cultured MSC products undergo laboratory expansion and are regulated as biologic drugs.
Potential risks include infection, inflammatory reactions, product variability, and exposure to products that have not undergone FDA review for safety and efficacy.
PRP and BMAC are typically autologous procedures performed using a patient's own tissues during the same procedure, whereas amniotic products are donor-derived biologic products distributed commercially.
No. A certificate of analysis may document certain lot-release tests, but it does not prove FDA approval, clinical effectiveness, lawful orthopedic marketing, or sterility at the time of injection.
Yes. Even if contamination occurred during manufacturing, the treating clinician may still face claims related to product selection, informed consent, marketing representations, and post-procedure care.
Liveyon distributed umbilical cord blood-derived products that were later associated with serious bacterial infections. CDC and FDA investigations reported infections in multiple patients, including bloodstream and joint infections, and FDA warned that these products were not lawfully marketed for those uses.
Berger DR, Centeno CJ, Kisiday JD, McIlwraith CW, Steinmetz NJ. Colony Forming Potential and Protein Composition of Commercial Umbilical Cord Allograft Products in Comparison With Autologous Orthobiologics. Am J Sports Med. 2021 Oct;49(12):3404-3413. doi: 10.1177/03635465211031275. Epub 2021 Aug 16. PMID: 34398643.
Binte Atique F, Ahmed KT, Asaduzzaman SM, Hasan KN. Effects of gamma irradiation on bacterial microflora associated with human amniotic membrane. Biomed Res Int. 2013;2013:586561. doi: 10.1155/2013/586561. Epub 2013 Aug 26. PMID: 24063009; PMCID: PMC3770025.
Dulugiac M, Moldovan L, Zarnescu O. Comparative studies of mesenchymal stem cells derived from different cord tissue compartments - The influence of cryopreservation and growth media. Placenta. 2015 Oct;36(10):1192-203. doi: 10.1016/j.placenta.2015.08.011. Epub 2015 Aug 29. PMID: 26343950.
Finnoff JT, Awan TM, Borg-Stein J, Harmon KG, Herman DC, Malanga GA, Master Z, Mautner KR, Shapiro SA. American Medical Society for Sports Medicine Position Statement: Principles for the Responsible Use of Regenerative Medicine in Sports Medicine. Clin J Sport Med. 2021 Nov 1;31(6):530-541. doi: 10.1097/JSM.0000000000000973. PMID: 34704973.
Fortier LA, Cercone M, Keller LE, Delco ML, Becktell L, Wells KV. Amnion and Umbilical Cord-Derived Products in Sports Medicine: From Basic Science to Clinical Application. Am J Sports Med. 2021 Jun;49(7):1954-1961. doi: 10.1177/03635465211010466. Epub 2021 Apr 30. PMID: 33929908.
Harrell CR, Djonov V, Fellabaum C, Volarevic V. Risks of Using Sterilization by Gamma Radiation: The Other Side of the Coin. Int J Med Sci. 2018 Jan 18;15(3):274-279. doi: 10.7150/ijms.22644. PMID: 29483819; PMCID: PMC5820857.
Koob TJ, Lim JJ, Massee M, Zabek N, Denozière G. Properties of dehydrated human amnion/chorion composite grafts: Implications for wound repair and soft tissue regeneration. J Biomed Mater Res B Appl Biomater. 2014 Aug;102(6):1353-62. doi: 10.1002/jbm.b.33141. Epub 2014 Mar 25. PMID: 24664953.
Moraes JTGO, Costa MM, Alves PCS, Sant'Anna LB. Effects of Preservation Methods in the Composition of the Placental and Reflected Regions of the Human Amniotic Membrane. Cells Tissues Organs. 2021;210(1):66-76. doi: 10.1159/000515448. Epub 2021 May 19. PMID: 34010831.
Panero AJ, Hirahara AM, Andersen WJ, Rothenberg J, Fierro F. Are Amniotic Fluid Products Stem Cell Therapies? A Study of Amniotic Fluid Preparations for Mesenchymal Stem Cells With Bone Marrow Comparison. Am J Sports Med. 2019 Apr;47(5):1230-1235. doi: 10.1177/0363546519829034. Epub 2019 Mar 7. PMID: 30844295.
Pegg DE. Principles of cryopreservation. Methods Mol Biol. 2015;1257:3-19. doi: 10.1007/978-1-4939-2193-5_1. PMID: 25428001.
Pogozhykh D, Prokopyuk V, Pogozhykh O, Mueller T, Prokopyuk O. Influence of Factors of Cryopreservation and Hypothermic Storage on Survival and Functional Parameters of Multipotent Stromal Cells of Placental Origin. PLoS One. 2015 Oct 2;10(10):e0139834. doi: 10.1371/journal.pone.0139834. PMID: 26431528; PMCID: PMC4592233.
Wagner M, Walter P, Salla S, Johnen S, Plange N, Rütten S, Goecke TW, Fuest M. Cryopreservation of amniotic membrane with and without glycerol additive. Graefes Arch Clin Exp Ophthalmol. 2018 Jun;256(6):1117-1126. doi: 10.1007/s00417-018-3973-1. Epub 2018 Apr 5. PMID: 29623460.
Whaley D, Damyar K, Witek RP, Mendoza A, Alexander M, Lakey JR. Cryopreservation: An Overview of Principles and Cell-Specific Considerations. Cell Transplant. 2021 Jan-Dec;30:963689721999617. doi: 10.1177/0963689721999617. PMID: 33757335; PMCID: PMC7995302.
Wolbank S, Hildner F, Redl H, van Griensven M, Gabriel C, Hennerbichler S. Impact of human amniotic membrane preparation on release of angiogenic factors. J Tissue Eng Regen Med. 2009 Dec;3(8):651-4. doi: 10.1002/term.207. PMID: 19701933.
Learn how ultrasound-guided percutaneous fasciotomy may revolutionize treatment for chronic exertional compartment syndrome with faster recovery and smaller incisions.
Read MoreResearchers used artificial intelligence and natural language processing to identify Shoulder Injury Related to Vaccine Administration (SIRVA) cases from over 3.7 million vaccinations. Learn what the study found, how
Read More