Email: info@BSBortho.com
Shoulder Injury Related to Vaccine Administration (SIRVA) has become one of the most discussed vaccine-related injuries over the last decade. While SIRVA remains relatively uncommon, it now accounts for the majority of claims filed through the National Vaccine Injury Compensation Program (VICP). Yet despite growing recognition of the condition, one major challenge has remained: accurately identifying SIRVA cases within large healthcare systems.
A 2022 study published in JMIR Public Health and Surveillance addressed this problem using artificial intelligence and natural language processing (NLP) to identify potential SIRVA cases across millions of vaccination records (Zheng et al, 2022). The findings provide some of the strongest population-level evidence to date regarding the frequency and characteristics of SIRVA.
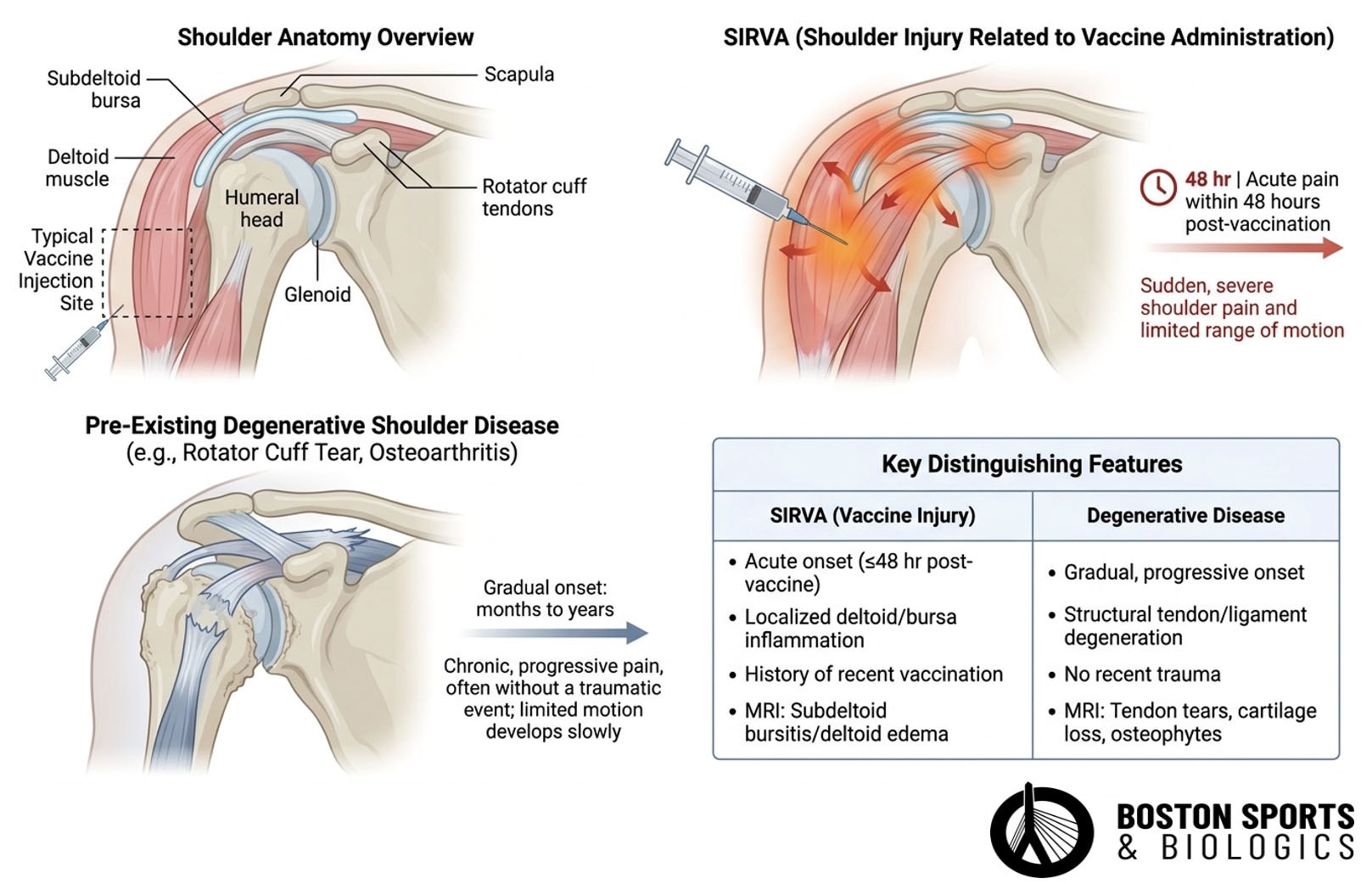
SIRVA refers to shoulder pain and dysfunction that develops after vaccine administration due to unintended injury of shoulder structures such as the subdeltoid bursa, rotator cuff tendons, or joint capsule. Learn more about SIRVA here.
SIRVA is characterized as a clinical syndrome rather than a specific diagnosis, as stated by the National Academies of Science, Engineering, and Medicine (NASEM) in their 2024 review (Miller et al, 2026). It is postulated to be an immune-mediated inflammatory response to vaccine antigen injected into or near the subacromial bursae or synovium, leading to shoulder pain and dysfunction (MacMahon et al, 2022).
NASEM established a causal relationship between vaccine administration and four specific diagnoses:
These injuries are "due to injection into the tissue resulting in the damage, and unlike the expected soreness that commonly follows vaccination, SIRVA is believed to result from improper injection technique, such as:
In a systematic review of COVID-19 vaccination-related SIRVA cases, 100% of patients reported pain and 90.1% described multiple symptoms (Fortier et al, 2024). Patients frequently report:
Because many shoulder conditions are common in the general population, distinguishing true SIRVA from coincidental shoulder pathology has historically been difficult.
Unlike conditions such as diabetes or pneumonia, SIRVA does not have its own dedicated ICD diagnostic code. As a result, researchers cannot simply search medical records for a diagnosis labeled "SIRVA." The AAOS has characterized SIRVA as "a medicolegal term rather than a true diagnosis," introduced in 2010 by the Vaccine Injury Compensation Program (Wiesel & Keeling, 2021).
Because SIRVA is a syndrome encompassing multiple shoulder pathologies rather than a single codifiable entity, it cannot be directly queried in electronic health records or claims databases using a single diagnostic code. Instead, patients may be diagnosed with:
Identifying whether these diagnoses were actually related to vaccination traditionally required labor-intensive manual chart review.
This limitation has made large-scale epidemiologic studies difficult and has contributed to ongoing debates regarding the true incidence of SIRVA.
Researchers from Kaiser Permanente Southern California and the CDC developed an advanced natural language processing (NLP) algorithm capable of reviewing clinical notes and identifying characteristics consistent with SIRVA (Zheng et al, 2022).
Rather than relying solely on diagnosis codes, the system analyzed physician documentation to identify:
The NLP system reviewed more than 4.2 million clinical notes associated with over 53,000 patients who developed shoulder-related diagnoses after vaccination.
For this study, a SIRVA case required:
This definition was modified from the Vaccine Injury Compensation Program criteria to make it practical for large-scale population research. The Vaccine Injury Compensation Program's definition for SIRVA, as applied in VAERS surveillance studies, requires: symptom onset within 48 hours after vaccine receipt, occurring after vaccination injected into the upper arm, with pain and decreased range of motion occurring in the vaccinated arm, and with no other abnormalities or prior history that could explain the symptoms (Miller et al, 2026). The VAERS study by Miller et al. added the requirement that symptoms last a minimum of 7 days to help differentiate SIRVA from normal injection site pain (Miller et al, 2026).
The investigators began with more than:
Using NLP, they identified 467 potential SIRVA cases. After physician chart review, 371 cases were confirmed.
The authors estimated approximately:
1 SIRVA case per 10,000 vaccinations
This finding is significant because previous estimates were largely derived from case reports, legal claims, or passive reporting systems such as VAERS. The study provides a population-based estimate using real-world healthcare data.
One of the most important findings was symptom timing.
Among confirmed SIRVA cases:
This supports one of the hallmark features used clinically and legally to distinguish SIRVA from unrelated shoulder pathology.
For clinicians evaluating potential SIRVA cases, a delayed onset weeks or months after vaccination would generally be less consistent with the pattern observed in this study.
The study found that symptoms frequently persisted for extended periods.
Among confirmed cases:
These findings reinforce that SIRVA is not simply transient post-vaccination soreness but may represent a prolonged musculoskeletal injury requiring medical treatment.
The study found that many clinical notes specifically attributed symptoms to vaccine administration.
Researchers identified:
Examples included provider statements suggesting rotator cuff irritation or bursitis related to vaccine administration. These findings support the theory that at least a subset of cases may result from mechanical injury caused by improper injection placement.
This study has several important implications.
Patients experiencing persistent shoulder pain shortly after vaccination may benefit from early evaluation, particularly when symptoms:
The research highlights the importance of:
The study demonstrates that artificial intelligence can identify rare vaccine-related adverse events efficiently and accurately, reducing reliance on costly manual chart review.
The findings provide objective epidemiologic data supporting several commonly cited characteristics of SIRVA:
These factors are frequently central to vaccine injury litigation and expert witness testimony.
This landmark study demonstrates that SIRVA can be identified in large healthcare databases using advanced natural language processing techniques. Among more than 3.7 million vaccinations, researchers identified 371 confirmed cases, corresponding to an estimated incidence of approximately 1 case per 10,000 vaccinations. Most patients developed symptoms within 48 hours, and many experienced prolonged shoulder dysfunction lasting months.
For clinicians, patients, and legal professionals alike, the study provides valuable evidence regarding the epidemiology and clinical presentation of SIRVA. As research continues to evolve, artificial intelligence may play an increasingly important role in improving our understanding of vaccine-related shoulder injuries and distinguishing them from coincidental degenerative shoulder conditions.
This study estimated approximately 1 SIRVA case per 10,000 vaccinations, making it uncommon but not exceedingly rare.
In this study, over 93% of confirmed cases developed symptoms within 2 days of vaccination.
No. SIRVA can include bursitis, rotator cuff pathology, adhesive capsulitis, tendinopathy, and other shoulder disorders occurring after vaccination.
No. AI cannot diagnose SIRVA directly. In this study, NLP was used to identify potential cases that were subsequently confirmed through physician chart review.
The study demonstrates an association between vaccination and a subset of shoulder injuries meeting SIRVA criteria. However, the authors note that proving direct causation remains challenging and requires careful evaluation of alternative explanations.
Yes. Degenerative rotator cuff disease, arthritis, adhesive capsulitis, and other shoulder disorders may coexist or be mistaken for SIRVA. Careful assessment of symptom timing, prior history, imaging findings, and clinical course is necessary to distinguish the two.
(781) 591-7855
20 Walnut St
Suite 14
Wellesley MA 02481
Fortier LM, Smith KL, Ina JG, Sinkler MA, Calcei JG, Salata MJ, Gillespie R, Voos JE. Common characteristics of shoulder injury related to vaccine administration following COVID-19 vaccination: a comprehensive systematic review. J Shoulder Elbow Surg. 2024 Jan;33(1):202-209. doi: 10.1016/j.jse.2023.07.040. Epub 2023 Sep 3. PMID: 37660886.
MacMahon A, Nayar SK, Srikumaran U. What Do We Know About Shoulder Injury Related to Vaccine Administration? An Updated Systematic Review. Clin Orthop Relat Res. 2022 Jul 1;480(7):1241-1250. doi: 10.1097/CORR.0000000000002181. Epub 2022 Mar 24. PMID: 35323136; PMCID: PMC9191332.
Miller ER, Marquez P, Aynalem G, et al. Atypical Shoulder Pain and Dysfunction After Vaccinations Reported to the Vaccine Adverse Event Reporting System (VAERS) January 1, 2018, Through October 31, 2022. Pharmacoepidemiology and Drug Safety 2026; 35(6):e70397. doi: 10.1002/pds.70397.
Wiesel BB, Keeling LE. Shoulder Injury Related to Vaccine Administration. J Am Acad Orthop Surg. 2021 Sep 1;29(17):732-739. doi: 10.5435/JAAOS-D-21-00021. PMID: 34185028.
Zheng C, Duffy J, Liu IA, Sy LS, Navarro RA, Kim SS, Ryan DS, Chen W, Qian L, Mercado C, Jacobsen SJ. Identifying Cases of Shoulder Injury Related to Vaccine Administration (SIRVA) in the United States: Development and Validation of a Natural Language Processing Method. JMIR Public Health Surveill. 2022 May 24;8(5):e30426. doi: 10.2196/30426. PMID: 35608886; PMCID: PMC9175103.
Learn how ultrasound-guided percutaneous fasciotomy may revolutionize treatment for chronic exertional compartment syndrome with faster recovery and smaller incisions.
Read MoreResearchers used artificial intelligence and natural language processing to identify Shoulder Injury Related to Vaccine Administration (SIRVA) cases from over 3.7 million vaccinations. Learn what the study found, how
Read More