Email: info@BSBortho.com
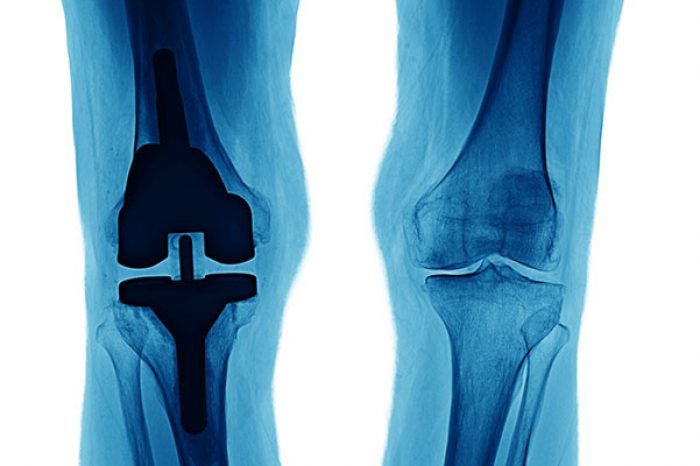
If you’ve been told you have knee osteoarthritis and are trying to avoid or delay a total knee replacement, you are not alone. Millions of Americans live with knee arthritis pain, stiffness, swelling, and limited mobility, learn more here.
But what if the key to slowing arthritis isn’t just inside the joint — but inside the bone beneath it?
A landmark randomized controlled trial published in International Orthopaedics by Hernigou et al. followed patients for 15 years and compared two different ways of delivering bone marrow concentrate (BMC) — commonly referred to as stem cell therapy — for knee osteoarthritis.
For decades, knee arthritis was thought to be a “wear-and-tear” cartilage problem. We now know it’s much more complex.
Osteoarthritis affects the cartilage, synovium (joint lining), and subchondral bone (bone beneath the cartilage.
Advanced imaging studies show that bone marrow lesions (BMLs) — areas of stress and inflammation inside the bone — are strongly linked to pain progression and structural damage. Learn more about bone marrow lesions here.
In fact, subchondral bone abnormalities may drive cartilage degeneration — not just the other way around (Hügle & Geurts, 2017).
That insight changes how we think about treatment.
In this prospective randomized trial, 60 patients with bilateral knee osteoarthritis received:
Intra-articular injection of bone marrow concentrate in one knee (into the joint space), and
Subchondral bone injection in the other knee (directly into the bone beneath the cartilage)
Each knee received the same number of mesenchymal stem cells (MSCs). The only difference was where the cells were delivered.
Patients were followed for:
2 years (clinical and MRI outcomes)
15 years (need for knee replacement)
This design allowed a true head-to-head comparison.
Pain Relief
Both groups improved initially. However, by 24 months:
Significant continued pain relief in the subchondral group
Pain relief started to fade in the intra-articular group
MRI Findings
Subchondral injections led to:
Regression of bone marrow lesions
Reduction in synovitis
Preservation (and slight increase) in cartilage volume
Intra-articular injections:
Did not reduce bone marrow lesions
Showed worsening synovitis
Showed continued cartilage loss
These findings suggests that targeting the bone with bone marrow derived mesenchymal stem cells may interrupt the disease process more effectively.
At the 15-year follow-up:
20% of subchondral-treated knees required knee replacement
70% of intra-articular-treated knees required knee replacement
Bone marrow lesions correlate strongly with:
Pain severity (Aso et al, 2021)
Structural progression (Driban et al, 2013; Moradi et al, 2021)
Risk of knee replacement (Tanamas et al, 2010)
Reducing BMLs may directly reduce symptoms and disease progression.
Mesenchymal stem cells in synovial fluid are barely detectable in healthy volunteers but increased in osteoarthritis. Research shows that mesenchymal stem cells are naturally present in synovial fluid in early osteoarthritis. If stem cells are already in the joint, adding more may have limited long-term impact (Sekiya et al, 2012).
However, subchondral bone-derived mesenchymal stem cells show evidence of exhaustion in primary osteoarthritis, with decreased viability and reduced osteogenic and chondrogenic potential compared to dysplastic OA. What does this mean? In osteoarthritis, subchondral bone may have
Fewer functional progenitor cells (Čamernik et al, 2020)
Age-related decline in MSC numbers (Zupan et al, 2021; Chandra et al, 2025)
Delivering cells directly into the bone may correct this deficiency.
Cartilage health depends on underlying bone integrity. Subchondral bone remodeling is recognized as integral to the progression of osteoarthritis (Hu et al, 2021; Delsmann et al, 2024).
By improving bone biology:
Inflammation may decrease
Mechanical stress may normalize
Cartilage degeneration may slow
No.
Most commonly advertised stem cell injections are intra-articular, not image-guided into bone and not targeting bone marrow lesions.
The technique used in this study involved:
Bone marrow aspiration from the iliac crest
Concentration of MSCs
Guided injection into specific subchondral regions
This is a highly targeted procedure, learn more about bone marrow derived mesenchymal stem cells here.

Based on the study findings:
Best candidates likely include:
Mild to moderate osteoarthritis (KL grades 1–3)
Presence of bone marrow lesions on MRI
Patients seeking to delay knee replacement
More advanced arthritis (KL grade 4), older age, and higher body weight increased risk of eventual knee replacement
If you have knee arthritis and are considering biologic treatment options, this study suggests:
Targeting bone marrow lesions may be more important than injecting into the joint alone
Addressing subchondral bone may slow structural progression
Some patients may meaningfully delay knee replacement
It does not mean knee replacement should be avoided when necessary. Total knee arthroplasty remains highly effective. But many patients seek ways to delay surgery — especially younger, active individuals.
This study suggests we may need to think beyond cartilage.
Aso K, Shahtaheri SM, McWilliams DF, Walsh DA. Association of subchondral bone marrow lesion localization with weight-bearing pain in people with knee osteoarthritis: data from the Osteoarthritis Initiative. Arthritis Res Ther. 2021 Jan 19;23(1):35. doi: 10.1186/s13075-021-02422-0. PMID: 33468243; PMCID: PMC7816469.
Čamernik K, Mihelič A, Mihalič R, Marolt Presen D, Janež A, Trebše R, Marc J, Zupan J. Increased Exhaustion of the Subchondral Bone-Derived Mesenchymal Stem/ Stromal Cells in Primary Versus Dysplastic Osteoarthritis. Stem Cell Rev Rep. 2020 Aug;16(4):742-754. doi: 10.1007/s12015-020-09964-x. PMID: 32200505.
Chandra A, Law SF, Pignolo RJ. Changing landscape of hematopoietic and mesenchymal cells and their interactions during aging and in age-related skeletal pathologies. Mech Ageing Dev. 2025 Jun;225:112059. doi: 10.1016/j.mad.2025.112059. Epub 2025 Apr 10. PMID: 40220914; PMCID: PMC12103995.
Delsmann J, Eissele J, Simon A, Alimy AR, von Kroge S, Mushumba H, Püschel K, Busse B, Ries C, Amling M, Beil FT, Rolvien T. Alterations in compositional and cellular properties of the subchondral bone are linked to cartilage degeneration in hip osteoarthritis. Osteoarthritis Cartilage. 2024 May;32(5):535-547. doi: 10.1016/j.joca.2024.01.007. Epub 2024 Feb 23. PMID: 38403152.
Driban JB, Price L, Lo GH, Pang J, Hunter DJ, Miller E, Ward RJ, Eaton CB, Lynch JA, McAlindon TE. Evaluation of bone marrow lesion volume as a knee osteoarthritis biomarker--longitudinal relationships with pain and structural changes: data from the Osteoarthritis Initiative. Arthritis Res Ther. 2013;15(5):R112. doi: 10.1186/ar4292. PMID: 24020939; PMCID: PMC3978948.
Hernigou P, Bouthors C, Bastard C, Flouzat Lachaniette CH, Rouard H, Dubory A. Subchondral bone or intra-articular injection of bone marrow concentrate mesenchymal stem cells in bilateral knee osteoarthritis: what better postpone knee arthroplasty at fifteen years? A randomized study. Int Orthop. 2021 Feb;45(2):391-399. doi: 10.1007/s00264-020-04687-7. Epub 2020 Jul 2. PMID: 32617651.
Hügle T, Geurts J. What drives osteoarthritis?-synovial versus subchondral bone pathology. Rheumatology (Oxford). 2017 Sep 1;56(9):1461-1471. doi: 10.1093/rheumatology/kew389. PMID: 28003493.
Hu W, Chen Y, Dou C, Dong S. Microenvironment in subchondral bone: predominant regulator for the treatment of osteoarthritis. Ann Rheum Dis. 2021 Apr;80(4):413-422. doi: 10.1136/annrheumdis-2020-218089. Epub 2020 Nov 6. PMID: 33158879; PMCID: PMC7958096.
Moradi K, Mohammadi S, Roemer FW, Momtazmanesh S, Hathaway Q, Ibad HA, Hunter DJ, Guermazi A, Demehri S. Progression of Bone Marrow Lesions and the Development of Knee Osteoarthritis: Osteoarthritis Initiative Data. Radiology. 2024 Sep;312(3):e240470. doi: 10.1148/radiol.240470. PMID: 39287521; PMCID: PMC11449232.
Sekiya I, Ojima M, Suzuki S, Yamaga M, Horie M, Koga H, Tsuji K, Miyaguchi K, Ogishima S, Tanaka H, Muneta T. Human mesenchymal stem cells in synovial fluid increase in the knee with degenerated cartilage and osteoarthritis. J Orthop Res. 2012 Jun;30(6):943-9. doi: 10.1002/jor.22029. Epub 2011 Dec 6. PMID: 22147634.
Tanamas SK, Wluka AE, Pelletier JP, Pelletier JM, Abram F, Berry PA, Wang Y, Jones G, Cicuttini FM. Bone marrow lesions in people with knee osteoarthritis predict progression of disease and joint replacement: a longitudinal study. Rheumatology (Oxford). 2010 Dec;49(12):2413-9. doi: 10.1093/rheumatology/keq286. Epub2010 Sep 7. PMID: 20823092.
Zupan J, Strazar K, Kocijan R, Nau T, Grillari J, Marolt Presen D. Age-related alterations and senescence of mesenchymal stromal cells: Implications for regenerative treatments of bones and joints. Mech Ageing Dev. 2021 Sep;198:111539. doi: 10.1016/j.mad.2021.111539. Epub 2021 Jul 7. PMID: 34242668.
Learn how ultrasound-guided percutaneous fasciotomy may revolutionize treatment for chronic exertional compartment syndrome with faster recovery and smaller incisions.
Read MoreResearchers used artificial intelligence and natural language processing to identify Shoulder Injury Related to Vaccine Administration (SIRVA) cases from over 3.7 million vaccinations. Learn what the study found, how
Read More