Email: info@BSBortho.com
Patellar tendinopathy is one of the most frustrating conditions affecting athletes, particularly those in jumping sports. Commonly known as jumper’s knee, the season prevalence reaches 19.0% in youth basketball players, with volleyball players showing the highest rates at 14.4% among non-elite athletes (Zwerver et al, 2011; Owoeye et al, 2021). In elite soccer, approximately 2.4% of players are affected each season (Hägglund et al, 2011).
The diagnosis is primarily clinical, characterized by activity-related anterior knee pain and tenderness at the lower pole of the patella (Malliaras et al, 2015; Theodorou et al, 2023). The hallmark features are pain localized to the inferior pole of the patella and load-related pain that increases with demand on the knee extensors, particularly in activities that store and release energy in the patellar tendon.
Despite its prevalence, patellar tendinopathy remains difficult to treat. Median symptom duration is substantial—83% of average total weeks of basketball exposure in affected players (Owoeye et al, 2021).
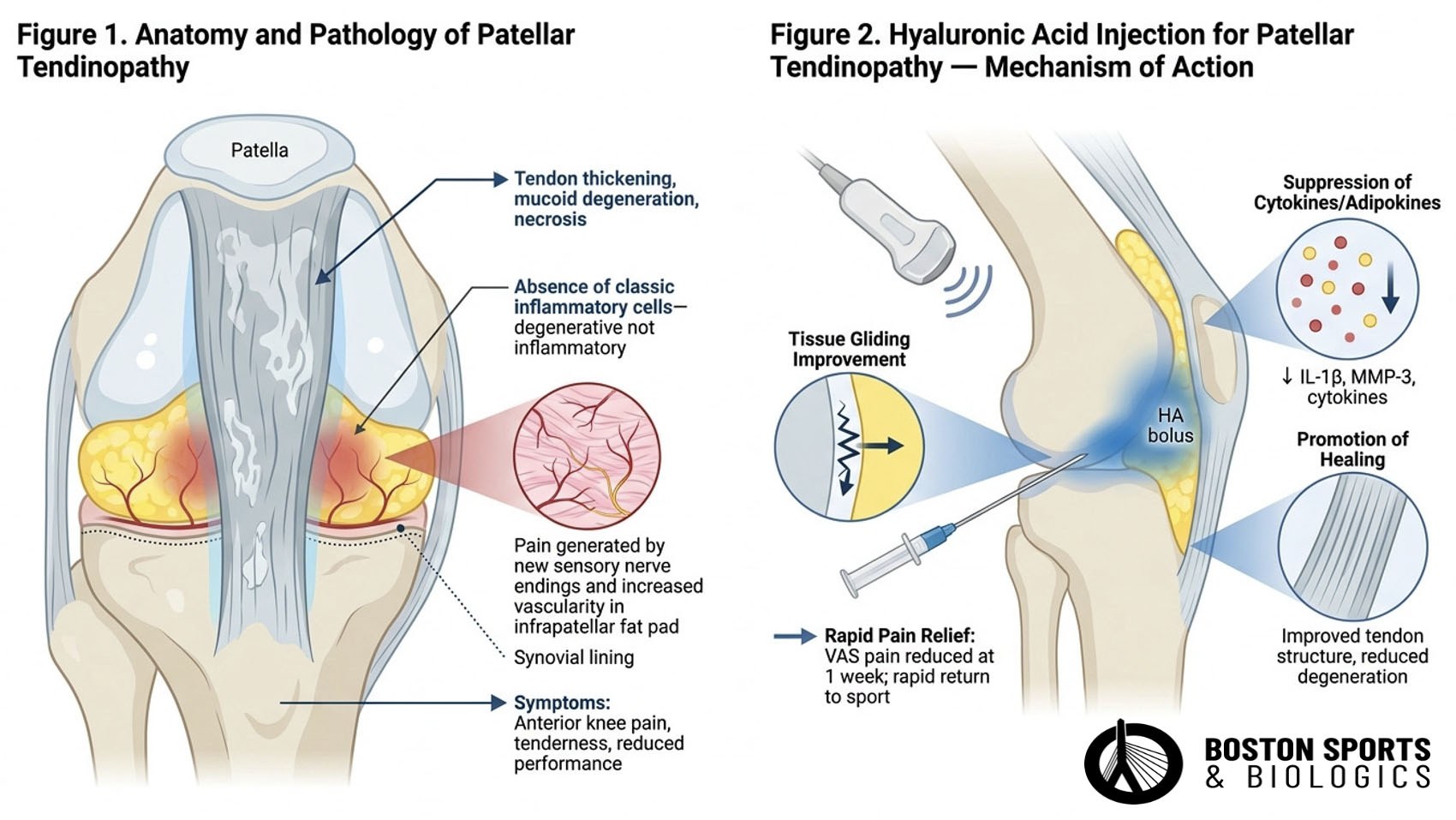
Patellar tendinopathy does not involve inflammation but rather represents microinjury to tendon fibers leading to mucoid degeneration, necrosis, and loss of transitional fibrocartilage, a degenerative process called tendinosis rather than tendinitis (Arner et al, 2024; Figueroa et al, 2016). This pathophysiologic understanding is critical, as it challenges the rationale for traditional anti-inflammatory approaches.
Patellar tendinopathy is a degenerative condition of the patellar tendon, often caused by repetitive loading, especially in sports involving jumping, sprinting, or rapid direction changes.
The pathology does not involve inflammation but rather represents microinjury to tendon fibers leading to mucoid degeneration, necrosis, and loss of transitional fibrocartilage. This occurs through repetitive or explosive movements that generate considerable loads and high peak strains across the patellar tendon (Marigi et al, 2022). Early pathogenesis represents a disturbed tissue homeostasis with fluid accumulation likely induced by repeated mechanical overloading rather than partial rupture (Tran et al, 2020).
Common symptoms include:
Imaging (MRI or ultrasound) may show:
Importantly, newer research highlights that pain may not come solely from the tendon itself. The infrapatellar fat pad, a highly innervated structure beneath the tendon, may play a significant role in pain generation.
The infrapatellar fat pad is an intracapsular, extrasynovial structure that is richly vascularized and innervated (Eymard & Chevalier, 2016; Dragoo et al, 2012). People with patellar tendinopathy have a significantly larger fat pad than healthy controls when controlled for height (Culvenor et al, 2011). In rat models of patellar tendinopathy, the infrapatellar fat pad shows greater cellularity, fibrosis, and vascularity compared to controls, with 38.2% fibrous area versus 11.2% in controls (Kitagawa et al, 2019).
Fibrotic changes in the infrapatellar fat pad induce new vessel formation and sensory nerve fiber endings that associate with prolonged pain (Onuma et al, 2020). The infrapatellar fat pad may contribute to pain not only through direct innervation but also via procatabolic and proinflammatory effects on its synovial lining (Eymard & Chevalier, 2016; .
Modern ultrasound can now assess potential pain generators located inside the patellar tendon-Hoffa fat pad interface, including the anterosuperior portion of the Hoffa body and the loose connective tissue of the deep paratenon with its microvascular plexus (Ricci et al, 2025).
The evidence confirms that traditional treatments often provide incomplete relief:
Rest and activity modification: While part of initial management, there is very low to low certainty evidence that conservative treatment improves pain or function compared to minimal intervention in short-term follow-up (Lopes et al, 2025; Mendonça et al, 2020)
NSAIDs: Despite being commonly used, the underlying pathology is degenerative rather than inflammatory, making the theoretical basis for NSAIDs questionable (Arner et al, 2024; Figueroa et al, 2016)
Physical therapy (eccentric exercises): While eccentric training is the most evidence-based conservative approach, showing 61% improvement in VISA scores, many patients remain refractory to this treatment (Vander Doelen & Jelley, 2020; Rosen et al, 2022; Everhart et al, 2017)
No clear consensus: Multiple systematic reviews confirm there is no clear evidence on the most effective approach to address patellar tendinopathy (Theodorou et al, 2023)
Hyaluronic acid (HA) is a naturally occurring substance in joints and connective tissues. It has been widely used in knee osteoarthritis and other musculoskeletal conditions due to its:
In tendon conditions, HA may:
Emerging evidence suggests that hyaluronic acid (HA) injections may offer a novel, minimally invasive option, particularly for athletes who have not responded to standard care.
In a case series of 50 athletic patients, HA injections resulted in 54% excellent outcomes (return to previous athletic activities with little difficulty) and 40% good outcomes (return with some limitation) (Muneta et al, 2012).
A single HA injection was placed into a very specific anatomical location, the interface between the posterior patellar tendon and the infrapatellar fat pad. Patients often experienced rapid improvement in pain during movement immediately after injection.
Patients reported a mean VAS pain reduction of 2.01 cm at 1 week in patellar tendinopathy patients. Notably, no patients stopped sports participation due to knee pain after treatment.
Hyaluronic acid injections appear to be very safe, with:
Compared to corticosteroids or surgery, HA maybe an appealing option for athletes seeking low-risk interventions.
HA may help reduce pain and support healing, but it is best used alongside rehabilitation
They work differently. HA may provide faster symptom relief, while PRP is more regenerative.
Most patients require 1–3 injections, depending on response.
Abate M, Schiavone C, Salini V. The use of hyaluronic acid after tendon surgery and in tendinopathies. Biomed Res Int. 2014;2014:783632. doi: 10.1155/2014/783632. Epub 2014 May 8. PMID: 24895610; PMCID: PMC4033484.
Arner JW, Kaeding CC, Bradley JP. Management of Patellar Tendinopathy. Arthroscopy. 2024 Jan;40(1):13-15. doi: 10.1016/j.arthro.2023.09.004. PMID: 38123261.
Chen WH, Lin CM, Huang CF, Hsu WC, Lee CH, Ou KL, Dubey NK, Deng WP. Functional Recovery in Osteoarthritic Chondrocytes Through Hyaluronic Acid and Platelet-Rich Plasma-Inhibited Infrapatellar Fat Pad Adipocytes. Am J Sports Med. 2016 Oct;44(10):2696-2705. doi: 10.1177/0363546516651822. Epub 2016 Jul 8. PMID: 27400716.
Culvenor AG, Cook JL, Warden SJ, Crossley KM. Infrapatellar fat pad size, but not patellar alignment, is associated with patellar tendinopathy. Scand J Med Sci Sports. 2011 Dec;21(6):e405-11. doi: 10.1111/j.1600-0838.2011.01334.x. Epub 2011 Jun 2. PMID: 21635562.
Dragoo JL, Johnson C, McConnell J. Evaluation and treatment of disorders of the infrapatellar fat pad. Sports Med. 2012 Jan 1;42(1):51-67. doi: 10.2165/11595680-000000000-00000. PMID: 22149697.
Everhart JS, Cole D, Sojka JH, Higgins JD, Magnussen RA, Schmitt LC, Flanigan DC. Treatment Options for Patellar Tendinopathy: A Systematic Review. Arthroscopy. 2017 Apr;33(4):861-872. doi: 10.1016/j.arthro.2016.11.007. Epub 2017 Jan 16. PMID: 28110807.
Eymard F, Chevalier X. Inflammation of the infrapatellar fat pad. Joint Bone Spine. 2016 Jul;83(4):389-93. doi: 10.1016/j.jbspin.2016.02.016. Epub 2016 Apr 7. PMID: 27068617.
Figueroa D, Figueroa F, Calvo R. Patellar Tendinopathy: Diagnosis and Treatment. J Am Acad Orthop Surg. 2016 Dec;24(12):e184-e192. doi: 10.5435/JAAOS-D-15-00703. PMID: 27855131.
Gervasi M, Barbieri E, Capparucci I, Annibalini G, Sisti D, Amatori S, Carrabs V, Valli G, Donati Zeppa S, Rocchi MBL, Stocchi V, Sestili P. Treatment of Achilles Tendinopathy in Recreational Runners with Peritendinous Hyaluronic Acid Injections: A Viscoelastometric, Functional, and Biochemical Pilot Study. J Clin Med. 2021 Mar 31;10(7):1397. doi: 10.3390/jcm10071397. PMID: 33807327; PMCID: PMC8037202.
Hägglund M, Zwerver J, Ekstrand J. Epidemiology of patellar tendinopathy in elite male soccer players. Am J Sports Med. 2011 Sep;39(9):1906-11. doi: 10.1177/0363546511408877. Epub 2011 Jun 3. PMID: 21642599.
Kitagawa T, Nakase J, Takata Y, Shimozaki K, Asai K, Tsuchiya H. Histopathological study of the infrapatellar fat pad in the rat model of patellar tendinopathy: A basic study. Knee. 2019 Jan;26(1):14-19. doi: 10.1016/j.knee.2018.07.016. Epub 2018 Aug 24. PMID: 30150068.
Lopes AD, Rizzo RR, Hespanhol L, Costa LO, Kamper SJ. Exercise for patellar tendinopathy. Cochrane Database Syst Rev. 2025 May 27;5(5):CD013078. doi: 10.1002/14651858.CD013078.pub2. PMID: 40421598; PMCID: PMC12107522.
Malliaras P, Cook J, Purdam C, Rio E. Patellar Tendinopathy: Clinical Diagnosis, Load Management, and Advice for Challenging Case Presentations. J Orthop Sports Phys Ther. 2015 Nov;45(11):887-98. doi: 10.2519/jospt.2015.5987. Epub 2015 Sep 21. PMID: 26390269.
Marigi EM, Buckley P, Razi F, Abbas MJ, Jildeh TR, Camp CL, Krych AJ, Okoroha KR. Patellar Tendinopathy: Critical Analysis Review of Current Nonoperative Treatments. JBJS Rev. 2022 Mar 8;10(3). doi: 10.2106/JBJS.RVW.21.00168. PMID: 35358114.
Mendonça LM, Leite HR, Zwerver J, Henschke N, Branco G, Oliveira VC. How strong is the evidence that conservative treatment reduces pain and improves function in individuals with patellar tendinopathy? A systematic review of randomised controlled trials including GRADE recommendations. Br J Sports Med. 2020 Jan;54(2):87-93. doi: 10.1136/bjsports-2018-099747. Epub 2019 Jun 6. PMID: 31171514.
Muneta T, Koga H, Ju YJ, Mochizuki T, Sekiya I. Hyaluronan injection therapy for athletic patients with patellar tendinopathy. J Orthop Sci. 2012 Jul;17(4):425-31. doi: 10.1007/s00776-012-0225-9. Epub 2012Apr 17.PMID: 22526713.
Onuma H, Tsuji K, Hoshino T, Inomata K, Udo M, Nakagawa Y, Katagiri H, Miyatake K, Watanabe T, Sekiya I, Muneta T, Koga H. Fibrotic changes in the infrapatellar fat pad induce new vessel formation and sensory nerve fiber endings that associate prolonged pain. J Orthop Res. 2020 Jun;38(6):1296-1306. doi: 10.1002/jor.24580. Epub 2020 Jan 10. PMID: 31903621.
Owoeye OBA, Palacios-Derflingher L, Pasanen K, HubkaRao T, Wiley P, Emery CA. The Burden and Risk Factors of Patellar and Achilles Tendinopathy in Youth Basketball: A Cohort Study. Int J Environ Res Public Health. 2021 Sep 8;18(18):9480. doi: 10.3390/ijerph18189480. PMID: 34574403; PMCID: PMC8470990.
Ricci V, Cocco G, Mezian K, Chang KV, Barbosa J, Naňka O, Özçakar L. Patellar tendon-Hoffa fat pad interface: From anatomy to high resolution ultrasound imaging. Knee. 2025 Jan;52:139-146. doi: 10.1016/j.knee.2024.10.024. Epub 2024 Nov 21. PMID: 39577112.
Rosen AB, Wellsandt E, Nicola M, Tao MA. Clinical Management of Patellar Tendinopathy. J Athl Train. 2022 Jul 1;57(7):621-631. doi: 10.4085/1062-6050-0049.21. PMID: 34623447; PMCID: PMC9528703.
Theodorou A, Komnos G, Hantes M. Patellar tendinopathy: an overview of prevalence, risk factors, screening, diagnosis, treatment and prevention. Arch Orthop Trauma Surg. 2023 Nov;143(11):6695-6705. doi: 10.1007/s00402-023-04998-5. Epub 2023 Aug 4. PMID: 37542006; PMCID: PMC10541843.
Tran PHT, Malmgaard-Clausen NM, Puggaard RS, Svensson RB, Nybing JD, Hansen P, Schjerling P, Zinglersen AH, Couppé C, Boesen M, Magnusson SP, Kjaer M. Early development of tendinopathy in humans: Sequence of pathological changes in structure and tissue turnover signaling. FASEB J. 2020 Jan;34(1):776-788. doi: 10.1096/fj.201901309R. Epub 2019 Nov 26. PMID: 31914656.
Vander Doelen T, Jelley W. Non-surgical treatment of patellar tendinopathy: A systematic review of randomized controlled trials. J Sci Med Sport. 2020 Feb;23(2):118-124. doi: 10.1016/j.jsams.2019.09.008. Epub 2019 Sep 13. PMID: 31606317.
Wu PT, Kuo LC, Su FC, Chen SY, Hsu TI, Li CY, Tsai KJ, Jou IM. High-molecular-weight hyaluronic acid attenuated matrix metalloproteinase-1 and -3 expression via CD44 in tendinopathy. Sci Rep. 2017 Jan 16;7:40840. doi: 10.1038/srep40840. PMID: 28091588; PMCID: PMC5238506.
Zwerver J, Bredeweg SW, van den Akker-Scheek I. Prevalence of Jumper's knee among nonelite athletes from different sports: a cross-sectional survey. Am J Sports Med. 2011 Sep;39(9):1984-8. doi: 10.1177/0363546511413370. Epub 2011 Jul 7. PMID: 21737835.
Learn how ultrasound-guided percutaneous fasciotomy may revolutionize treatment for chronic exertional compartment syndrome with faster recovery and smaller incisions.
Read MoreResearchers used artificial intelligence and natural language processing to identify Shoulder Injury Related to Vaccine Administration (SIRVA) cases from over 3.7 million vaccinations. Learn what the study found, how
Read More