Email: info@BSBortho.com
Shoulder pain following vaccination has become an increasingly recognized medical and legal issue over the past decade. The condition known as Shoulder Injury Related to Vaccine Administration (SIRVA) is now included within the National Vaccine Injury Compensation Program (VICP) and has generated thousands of claims. However, one of the greatest challenges facing physicians, attorneys, and patients is determining whether shoulder symptoms truly represent SIRVA or simply reflect previously existing degenerative shoulder disease that became symptomatic around the time of vaccination.
This distinction is critical. While SIRVA is considered an injury resulting from improper vaccine administration, degenerative shoulder conditions are extremely common in the general population and often exist long before symptoms develop. Understanding the differences can help guide diagnosis, treatment, and medico-legal evaluation.
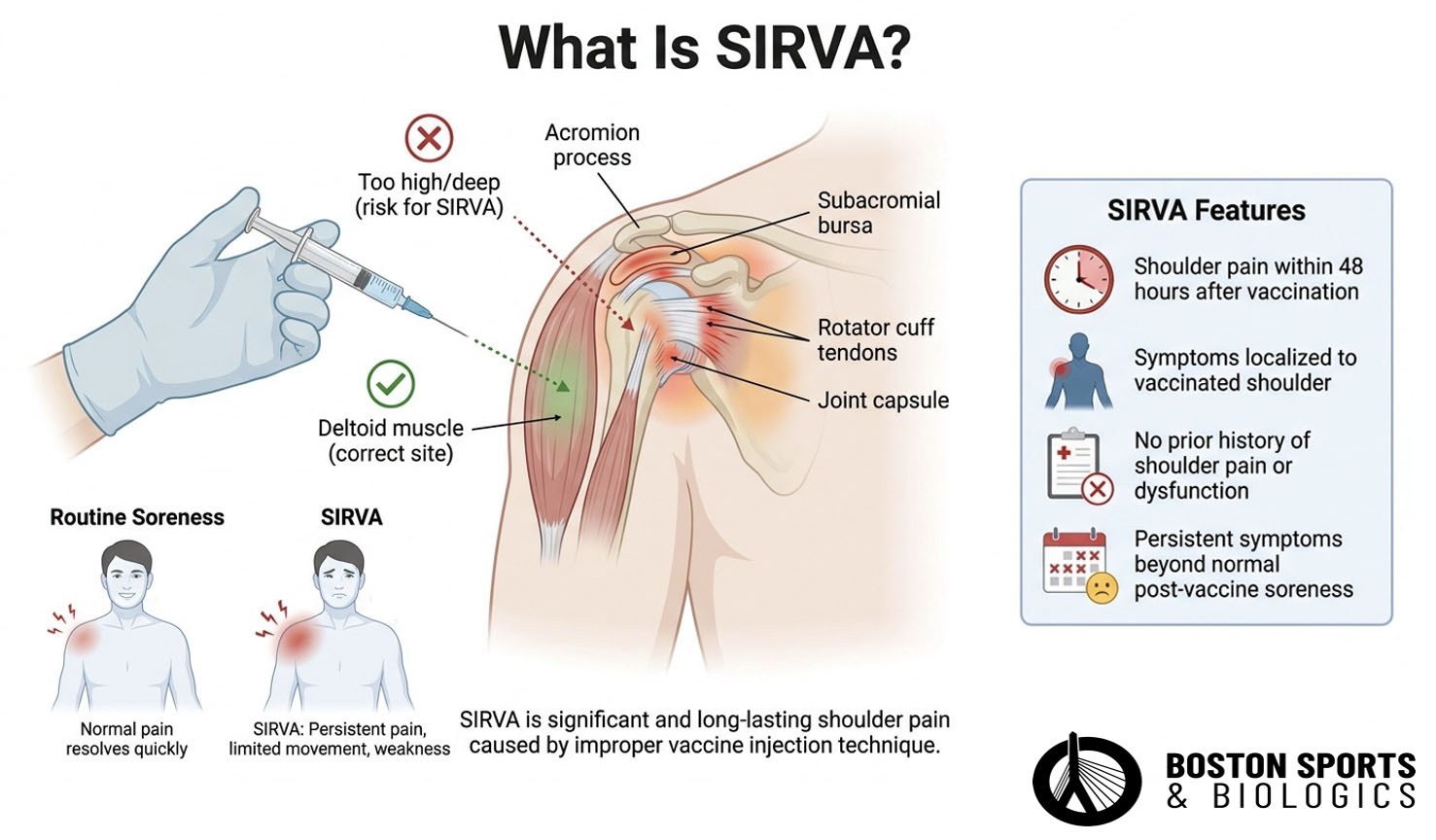
SIRVA refers to shoulder pain and dysfunction that occurs following vaccine administration, typically due to improper injection technique. Rather than being injected into the deltoid muscle, the vaccine may be delivered too high or too deep, resulting in inflammation of structures such as the subacromial bursa, rotator cuff tendons, joint capsule, or surrounding tissues (MacMahon et al, 2022; Miller et al, 2026).
It is notably described as a "medicolegal term rather than a true diagnosis." The AAOS review emphasizes that it was introduced in 2010 by the Vaccine Injury Compensation Program (VICP) after an increase in claims (Wiesel & Keeling, 2021). The 2024 National Academies of Science, Engineering, and Medicine (NASEM) review further clarified that SIRVA "represents a clinical syndrome, is not a specific diagnosis, and may have a number of causes."
The National Vaccine Injury Compensation Program generally recognizes several hallmark features:
Unlike routine post-vaccination soreness, SIRVA often results in significant pain, loss of range of motion, weakness, and functional limitations that may persist for months or years.
The incidence appears rare but likely underreported. MacMahon et al. estimated approximately 1 in 130,000 vaccination events based on the best available comparative study (MacMahon et al, 2022).
However, Janssen et al. (2023) found a much higher prevalence of 3.3% among Dutch hospital workers after COVID-19 vaccination when actively surveyed, with 56.2% of affected individuals still symptomatic at follow-up (Janssen et al, 2023). The CDC's Vaccine Safety Datalink estimated 7.78 additional cases of bursitis per million people vaccinated (Miller et al, 2026).
The difficulty arises because degenerative shoulder disease is extraordinarily common.
Numerous imaging studies have demonstrated that asymptomatic abnormalities are frequently present in individuals with no shoulder complaints. Rotator cuff tears, bursitis, tendinosis, labral degeneration, and arthritis become increasingly prevalent with age.
Prevalence of Rotator Cuff Pathology in Asymptomatic Shoulders
Research has shown that more than 50% of individuals over age 65 may have a rotator cuff tear visible on imaging, many without symptoms. The presence of these findings after vaccination does not necessarily prove that the vaccine caused the pathology.
Beyond the Rotator Cuff: Glenohumeral Joint Pathology
The SCRUTINY systematic review (Ibounig et al., 2024) found that the population-based prevalence of glenohumeral joint imaging abnormalities in asymptomatic individuals may range between 30% and 75%,including glenohumeral osteoarthritis (15–75%), labral abnormalities (20%), and long head of biceps tendon abnormalities (30%) (Ibounig et al, 2024).
The Diagnostic Dilemma: New Injury vs. Unmasked Pathology
The central diagnostic dilemma described, whether vaccination caused a new injury or simply drew attention to preexisting pathology, is a genuine and actively debated question in the literatureThe tension between these perspectives has direct clinical relevance. As Ibounig et al. recommend, clinicians should shift from asking "whether abnormalities exist" to "whether they plausibly explain the clinical findings," and consider adopting "more precise and less value-laden terminology," such as "structural alteration" or "degeneration" rather than "tear," to reduce overdiagnosis and unnecessary intervention (Ibounig et al, 2026).
Wright et al. (2023) further note that advanced imaging in SIRVA cases "rarely provided information that affected treatment," reinforcing the limited utility of imaging in this context (Wright et al, 2023).
1. Timing of Symptom Onset
One of the strongest indicators of SIRVA is the rapid onset of symptoms, and the VICP's Vaccine Injury Table specifies onset within 48 hours as a criterion for SIRVA claims (MacMahon et al, 2022; Wiesel & Keeling, 2021).
Most reported cases develop pain immediately or within 24 to 48 hours following vaccination. Some patients describe severe pain beginning during the injection itself.
In contrast, degenerative shoulder disease typically develops gradually over weeks, months, or years.
2. Absence of Prior Symptoms
Perhaps the most important criterion involves the patient's pre-vaccination shoulder status. The VICP criteria explicitly require no prior history of pain or dysfunction in the affected shoulder (Wright et al, 2023; Wiesel & Keeling, 2021).
Wright et al. (2023) confirmed in their systematic review that the absence of prior shoulder complaints is a key diagnostic feature, noting that SIRVA is defined partly by "no history of pain, inflammation, or dysfunction of the affected shoulder prior to vaccination" (Wright et al, 2023).
Questions to consider include:
The stronger the evidence that the shoulder was asymptomatic before vaccination, the stronger the argument for SIRVA.
3. Localization to the Vaccinated Shoulder
True SIRVA symptoms occur in the same shoulder that received the vaccine.
Patients often describe:
The symptoms are generally unilateral and directly correspond to the injection site.
MRI and ultrasound frequently identify abnormalities in patients suspected of having SIRVA, but imaging alone cannot establish causation.
Common imaging findings include:
The problem is that many of these findings are also common in degenerative shoulder disease.
Donners et al. (2023) found in a case series of 9 chronic SIRVA patients that the most common MRI findings were greater tuberosity erosions (89%), infraspinatus tendonitis (78%), capsulitis (56%), synovitis (56%), and bone marrow edema (56%). Notably, greater tuberosity erosions may be a more specific finding for SIRVA, as they are less commonly seen in typical degenerative disease (Donners et al, 2023).
Fortier et al. (2024) found that across 81 COVID-19 SIRVA cases, the most common diagnoses were bursitis (32.1%), adhesive capsulitis (27.2%), and rotator cuff tear or tendinopathy (21.0%) (Fortier et a, 2024).
Wright et al. (2023) importantly noted that advanced imaging in SIRVA cases "rarely provided information that affected treatment", reinforcing the limited utility of imaging for establishing causation (Wright et al, 2023).
For example, a 65-year-old patient with a rotator cuff tear on MRI may have had that tear for years before vaccination. The MRI cannot determine whether the tear was caused by the injection or merely discovered after symptoms developed.
Imaging cannot determine whether pathology was caused by the injection
or merely discovered afterward, and is the crux of the ongoing debate in
the literature, which is why imaging findings must always be interpreted alongside the clinical history.
Current evidence suggests that many patients who develop SIRVA symptoms may have underlying degenerative pathology that was previously asymptomatic.
Rather than creating a brand-new rotator cuff tear, the vaccine-related inflammatory response may aggravate pre-existing disease.
This concept is particularly important because:
The medical question often becomes whether vaccination caused a new injury or exacerbated an existing condition.
The proposed pathophysiology supports this concept: SIRVA is hypothesized to involve an immune-mediated inflammatory response to vaccine antigens injected into or near the subacromial bursa or synovium (Miller et al, 2026; Yuen et al, 2022). This local inflammatory cascade could plausibly irritate preexisting degenerative tissue that was previously quiescent.
The National Academies of Sciences, Engineering, and Medicine reviewed available evidence regarding vaccine administration injuries and concluded that improperly administered vaccines can produce local inflammatory reactions involving shoulder structures (Miller et al, 2026).
The NASEM review found a causal relationship between
vaccine administration and four specific diagnoses:
The report states that "these injuries are due to injection into the tissue resulting in the damage." Importantly, the NASEM also clarified that SIRVA "represents a clinical syndrome, is not a specific diagnosis, and may have a number of causes."
However, the report also acknowledged significant limitations in proving direct causation for many specific imaging findings. The available evidence supports an association between improper vaccine placement and shoulder injury, but distinguishing vaccine-induced pathology from naturally occurring degenerative disease remains challenging in many cases.
Several examination findings may help differentiate SIRVA from chronic degenerative disease.
Patients with SIRVA often demonstrate significant pain with shoulder motion, marked reduction in active range of motion, painful arc, and diffuse tenderness around the injection region are consistently documented.
Adhesive capsulitis-like stiffness is particularly common in some patients with SIRVA.
Conversely, longstanding degenerative disease may demonstrate:
The examination rarely provides a definitive answer but helps build the overall clinical picture.
Distinguishing SIRVA from pre-existing shoulder disease has implications beyond treatment.
The diagnosis may affect:
SIRVA remains a diagnosis based primarily on clinical history rather than imaging findings. The physical examination findings described for both SIRVA and chronic degenerative disease are accurate and well-supported. The key
distinguishing features are temporal: SIRVA presents with acute-onset pain, diffuse tenderness, and inflammatory restriction of motion, while chronic degenerative disease demonstrates insidious weakness, muscle atrophy, fatty infiltration, and often bilateral involvement.
The strongest evidence supporting SIRVA includes:
Because degenerative shoulder abnormalities are common, MRI findings alone cannot distinguish SIRVA from pre-existing disease. Instead, diagnosis requires integration of timing, symptoms, prior medical history, physical examination, and imaging findings.
For patients, physicians, and attorneys alike, understanding this distinction is essential when evaluating whether a vaccine-related shoulder injury truly represents SIRVA or the unmasking of previously silent degenerative disease.
Most cases develop within 48 hours of vaccination, often immediately or the same day. Delayed onset weeks later is generally less consistent with classic SIRVA.
No. MRI findings such as bursitis, tendinosis, or rotator cuff tears can occur in both SIRVA and age-related degenerative shoulder disease.
Yes. Many patients likely have underlying asymptomatic degenerative pathology that becomes symptomatic following vaccine-related inflammation.
The clinical history is usually more important than imaging. Rapid onset after vaccination and the absence of prior shoulder symptoms are among the strongest diagnostic clues.
Yes. SIRVA was added to the Vaccine Injury Table in 2017 and remains a recognized compensable injury when specific criteria are met.
Rotator cuff disease, adhesive capsulitis, glenohumeral arthritis, acromioclavicular joint arthritis, cervical radiculopathy, and calcific tendinopathy are among the most common alternative diagnoses.
Bass JR, Poland GA. Shoulder injury related to vaccine administration (SIRVA) after COVID-19 vaccination. Vaccine. 2022 Aug 12;40(34):4964-4971. doi: 10.1016/j.vaccine.2022.06.002. Epub 2022 Jun 8. PMID: 35817645; PMCID: PMC9174179.
Brown GA, Weber S, Chahla J, et al. Management of Rotator Cuff Injuries: Evidence-Based Clinical Practice Guideline. American Academy of Orthopaedic Surgeons. 2025. https://www.aaos.org/rccpg2025
Donners R, Gehweiler J, Kovacs B, Breit HC, Daikeler T, Harder D, Berger CT. Chronic stage magnetic resonance imaging findings in patients with shoulder injury related to vaccine administration (SIRVA). Skeletal Radiol. 2023 Sep;52(9):1695-1701. doi: 10.1007/s00256-023-04334-3. Epub 2023 Apr 3. PMID: 37012390; PMCID: PMC10069733.
Fortier LM, Smith KL, Ina JG, Sinkler MA, Calcei JG, Salata MJ, Gillespie R, Voos JE. Common characteristics of shoulder injury related to vaccine administration following COVID-19 vaccination: a comprehensive systematic review. J Shoulder Elbow Surg. 2024 Jan;33(1):202-209. doi: 10.1016/j.jse.2023.07.040. Epub 2023 Sep 3. PMID: 37660886.
Ghosh S, Pandey SK, Biswas A, Pandey J. Adhesive Capsulitis After COVID-19 Vaccination: A Case Series. Am J Phys Med Rehabil. 2023 Jun 1;102(6):e79-e82. doi: 10.1097/PHM.0000000000002194. Epub 2023 Jan 23. PMID: 36722847; PMCID: PMC10184708.
Hesse EM, Atanasoff S, Hibbs BF, Adegoke OJ, Ng C, Marquez P, Osborn M, Su JR, Moro PL, Shimabukuro T, Nair N. Shoulder Injury Related to Vaccine Administration (SIRVA): Petitioner claims to the National Vaccine Injury Compensation Program, 2010-2016. Vaccine. 2020 Jan 29;38(5):1076-1083. doi: 10.1016/j.vaccine.2019.11.032. Epub 2019 Nov 23. PMID: 31771864; PMCID: PMC9169064.
Ibounig T, Järvinen TLN, Raatikainen S, Härkänen T, Sillanpää N, Bensch F, Haapamäki V, Toivonen P, Björkenheim R, Ryösä A, Kanto K, Lepola V, Joukainen A, Paavola M, Koskinen S, Rämö L, Buchbinder R, Taimela S. Incidental Rotator Cuff Abnormalities on Magnetic Resonance Imaging. JAMA Intern Med. 2026 Apr 1;186(4):406-414. doi: 10.1001/jamainternmed.2025.7903. PMID: 41697693; PMCID: PMC12910452.]
Ibounig T, Sanders S, Haas R, Jones M, Järvinen TL, Taimela S, Docking S, Rämö L, Buchbinder R. Systematic Review of Shoulder Imaging Abnormalities in Asymptomatic Adult Shoulders (SCRUTINY): Abnormalities of the glenohumeral joint. Osteoarthritis Cartilage. 2024 Oct;32(10):1184-1196. doi: 10.1016/j.joca.2024.06.001. Epub 2024 Jun 12. PMID: 38876437.
Janssen ERC, van Montfoort AZ, Hollman F, Lambers Heerspink FO. The prevalence and clinical course of shoulder injury related to vaccine administration (SIRVA) after COVID-19 vaccines in Dutch hospital workers. Vaccine. 2023 Sep 22;41(41):6042-6047. doi: 10.1016/j.vaccine.2023.08.043. Epub 2023 Aug 25. PMID: 37635003.
MacMahon A, Nayar SK, Srikumaran U. What Do We Know About Shoulder Injury Related to Vaccine Administration? An Updated Systematic Review. Clin Orthop Relat Res. 2022 Jul 1;480(7):1241-1250. doi: 10.1097/CORR.0000000000002181. Epub 2022 Mar 24. PMID: 35323136; PMCID: PMC9191332.
Martín Arias LH, Sanz Fadrique R, Sáinz Gil M, Salgueiro-Vazquez ME. Risk of bursitis and other injuries and dysfunctions of the shoulder following vaccinations. Vaccine. 2017 Sep 5;35(37):4870-4876. doi: 10.1016/j.vaccine.2017.07.055. Epub 2017 Jul 31. PMID: 28774564.
Miller ER, Marquez P, Aynalem G, et al. Atypical Shoulder Pain and Dysfunction After Vaccinations Reported to the Vaccine Adverse Event Reporting System (VAERS) January 1, 2018, Through October 31, 2022. Pharmacoepidemiology and Drug Safety. Volume 35, Issue 6 e70397
Petrakis N, Addison M, Penak B, Schrader S, Mallard J, Clothier HJ, Buttery JP, Crawford NW, Cheng DR. Shoulder injury following COVID-19 vaccine administration: a case series and proposed diagnostic algorithm. Expert Rev Vaccines. 2023 Jan-Dec;22(1):299-306. doi:10.1080/14760584.2023.2189463. PMID: 36894495.
Sanders S, Ibounig T, Haas R, Jones M, Rämö L, Docking S, Järvinen T, Taimela S, Hoffmann T, Buchbinder R. Rotator Cuff Imaging Abnormalities in Asymptomatic Shoulders: A Systematic Review. J Orthop Sports Phys Ther. 2025 Dec;55(12):1-16. doi: 10.2519/jospt.2025.13611. PMID: 41308021.
Slette E, Rohrback M, Ring D. Persistent Shoulder Pain After Vaccine Administration Is Associated with Common Incidental Pathology: A Systematic Review. Clin Orthop Relat Res. 2022 Jul 1;480(7):1251-1258. doi: 10.1097/CORR.0000000000002191. Epub 2022 Mar 23. PMID: 35319515; PMCID: PMC9191317.
Wiesel BB, Keeling LE. Shoulder Injury Related to Vaccine Administration. J Am Acad Orthop Surg. 2021 Sep 1;29(17):732-739. doi: 10.5435/JAAOS-D-21-00021. PMID: 34185028.
Wright JO, Wiggins W, Smith MS, King JJ, Wright TW. Shoulder Pain and Dysfunction After Vaccination: A Systematic Review. JBJS Rev. 2023 Jan 12;11(1). doi: 10.2106/JBJS.RVW.22.00134. PMID: 36722836.
Yuen WLP, Loh SYJ, Wang DB. SIRVA (Shoulder Injury Related to Vaccine Administration) following mRNA COVID-19 Vaccination: Case discussion and literature review. Vaccine. 2022 Apr 20;40(18):2546-2550. doi: 10.1016/j.vaccine.2022.03.037. Epub 2022 Mar 21. PMID: 35339304; PMCID:
PMC8934720.
Learn how ultrasound-guided percutaneous fasciotomy may revolutionize treatment for chronic exertional compartment syndrome with faster recovery and smaller incisions.
Read MoreResearchers used artificial intelligence and natural language processing to identify Shoulder Injury Related to Vaccine Administration (SIRVA) cases from over 3.7 million vaccinations. Learn what the study found, how
Read More