Email: info@BSBortho.com
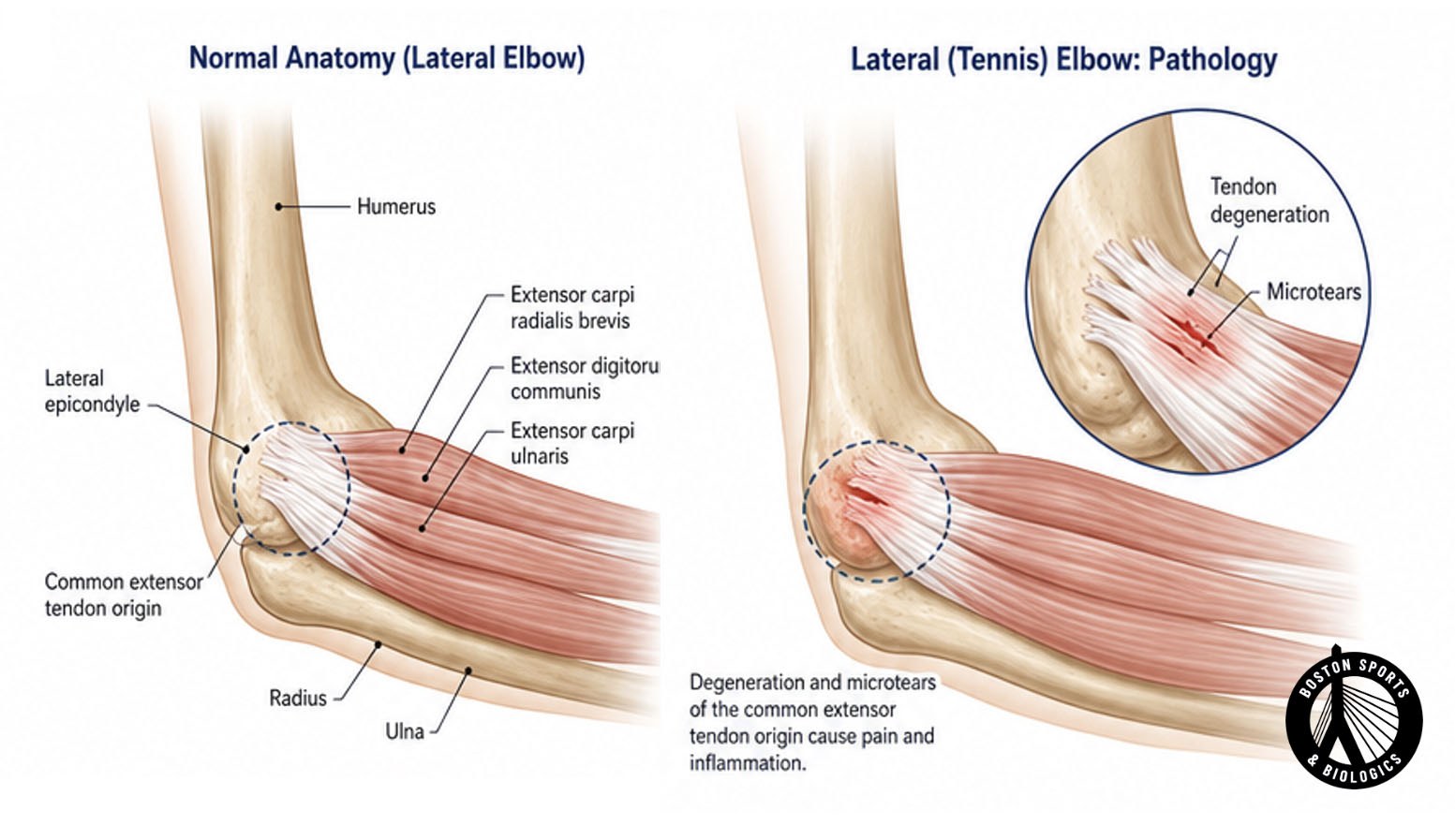
Lateral epicondylitis (tennis elbow) is thought to be caused by chronic degenerative change at the origin of the elbow extensor tendons, though the exact cause is not well understood.
Pathological evaluation has shown infiltration of fibroblasts, vascular hyperplasia, and disorganized collagen, a process termed angiofibroblastic tendinosis, rather than a primarily inflammatory condition [Wolf, 2023].
The condition is characterized by the insidious onset of lateral elbow pain, usually in the absence of trauma, and affects 1 to 3% of adults with peak prevalence among persons aged 40 to 49 years [Wolf, 2023].
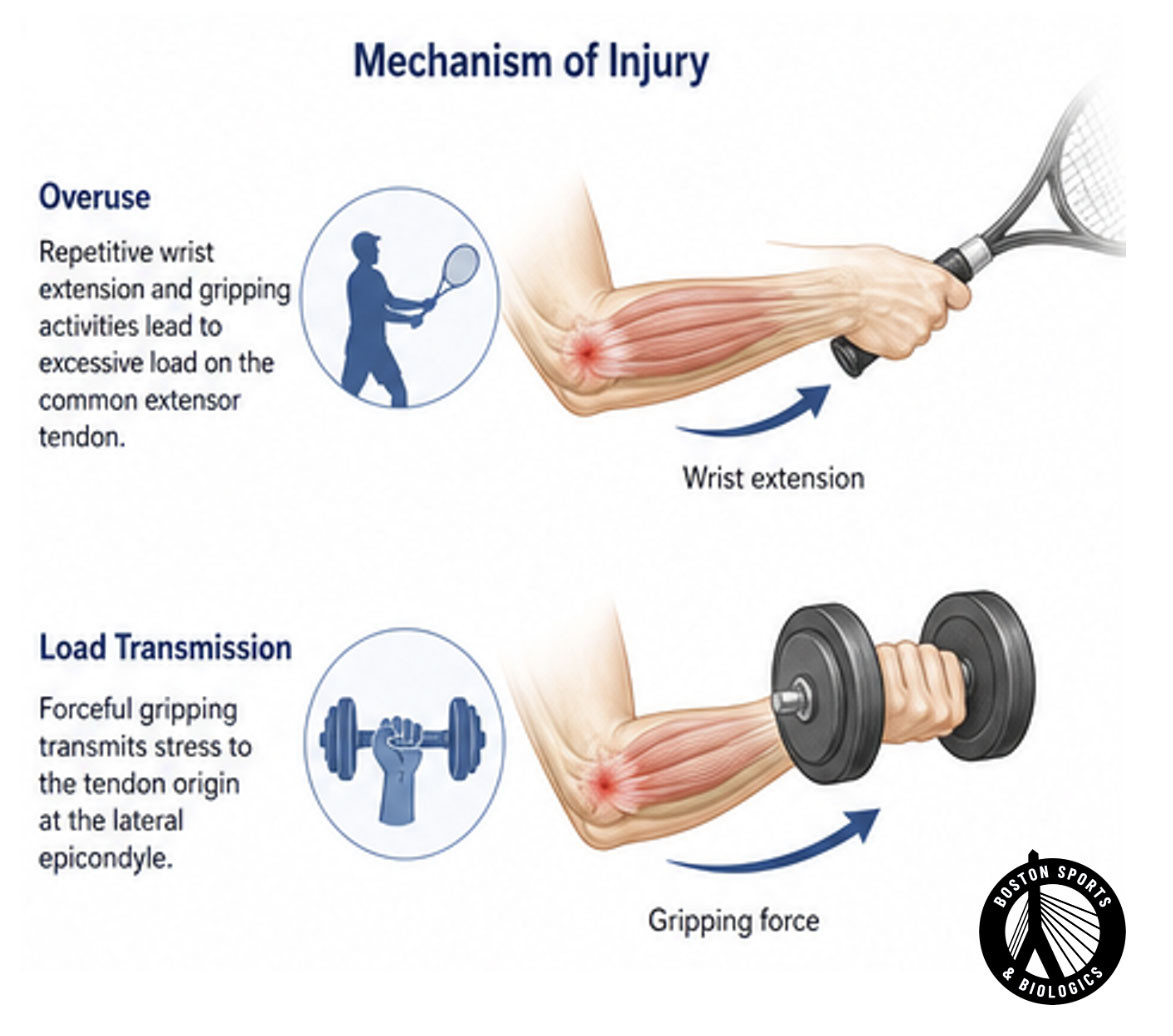
Risk factors for developing tennis elbow include repetitive occupational or athletic activities involving wrist extension and supination, as well as high physical load [Wolf, 2023; Tosti et al, 2013]. The condition is most prevalent among individuals aged 40 to 49 years [Wolf, 2023].

Tennis elbow, also known as lateral epicondylitis, is primarily diagnosed clinically.
Patients typically present with a gradual onset of lateral elbow pain without a history of trauma. Patients will typically report pain or burning over the outside of the elbow. Weak grip strength is common.
On physical examination, findings include tenderness at the lateral epicondyle of the distal humerus and pain or weakness with resisted wrist extension [Wolf, 2023].
Imaging studies include:
Plane radiographs (x-rays) can be ordered to rule out associated pathology, including osteoarthritis, but are not always required [Wolf, 2023].
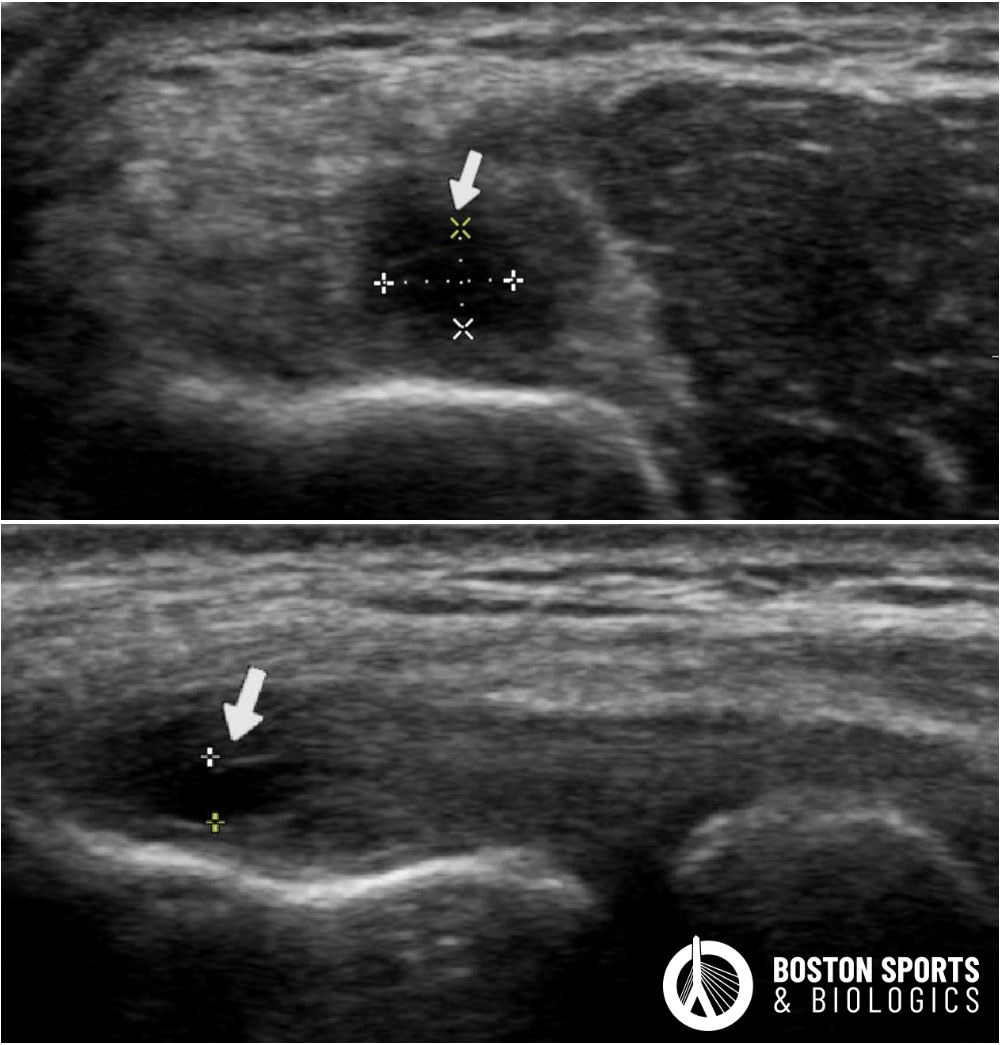
Diagnostic ultrasound can reveal tendon thickening, hypoechogenicity, and neovascularity and has a high
sensitivity (75%-100%) and specificity (85%-96%) [Karanasios et al, 2022; Keijsers, 2018].
Magnetic Resonance Imaging (MRI) is another option, particularly useful for identifying tendon thickening and enthesopathy, with sensitivity and specificity ranging from 81%-100% [Karanasios et al, 2022].
Surgery is considered for refractory cases that do not respond to nonoperative measures after 6-12 months:
Tennis elbow, also known as lateral epicondylitis or lateral elbow tendinopathy, is a condition caused by degeneration and microtearing of the tendons that attach to the outside of the elbow. Despite the name, most cases occur in people who have never played tennis and are related to repetitive gripping, lifting, typing, manual labor, or recreational activities.
Common symptoms include:
Tennis elbow develops when repetitive stress exceeds the tendon’s ability to heal. Common causes include:
Diagnosis is typically based on history, physical examination, and diagnostic ultrasound. Ultrasound can identify tendon thickening, degeneration, partial tears, calcifications, and increased blood flow associated with chronic tendinopathy. In some cases, MRI may be recommended if other conditions are suspected.
Some cases improve with activity modification, physical therapy, and time. However, symptoms can persist for months or even years when significant tendon degeneration is present. Chronic cases often require more targeted treatment to stimulate tendon healing.
Treatment options may include:
Corticosteroid injections may provide short-term pain relief, but multiple studies have demonstrated higher recurrence rates and poorer long-term outcomes compared with other treatments. They do not address the underlying tendon degeneration.
Platelet-rich plasma (PRP) uses concentrated platelets from your own blood to deliver growth factors that may stimulate tendon healing. PRP has been shown in multiple studies to improve pain and function in patients with chronic tennis elbow who have not responded to conservative treatment.
In most cases, yes. The goal is to modify activities that aggravate symptoms while maintaining overall fitness. A rehabilitation program can help identify exercises that promote healing while minimizing further tendon stress.
Patients with symptoms lasting longer than 3–6 months, persistent pain despite physical therapy, or ultrasound evidence of tendon degeneration may be candidates for regenerative treatments such as PRP or minimally invasive ultrasound-guided tendon procedures. A comprehensive evaluation can help determine the most appropriate treatment plan for your specific condition.
Hegmann KT, Hoffman HE,
Belcourt RM, Byrne K, Glass L, Melhorn JM, Richman J, Zinni P 3rd,
Thiese MS, Ott U, Tokita K, Passey DG, Effiong AC, Robbins RB, Ording
JA; American College of Occupational and Environmental Medicine. ACOEM
practice guidelines: elbow disorders. J Occup Environ Med. 2013
Nov;55(11):1365-74.
Hohmann E. Editorial
Commentary: Arthroscopic Debridement of Tennis Elbow Nonresponsive to
Nonoperative Measures Is a Good Option and Clinical Outcomes Are
Associated With Radiographic Outcomes. Arthroscopy. 2022
Dec;38(12):3130-3132.
Johnson GW,
Cadwallader K, Scheffel SB, Epperly TD. Treatment of lateral
epicondylitis. Am Fam Physician. 2007 Sep 15;76(6):843-8.
Keijsers R, de Vos RJ, Kuijer PPF, van den Bekerom MP, van der Woude HJ, Eygendaal D. Tennis elbow. Shoulder Elbow.2019 Oct;11(5):384-392.
Koh
JS, Mohan PC, Howe TS, Lee BP, Chia SL, Yang Z, Morrey BF. Fasciotomy
and surgical tenotomy for recalcitrant lateral elbow tendinopathy: early
clinical experience with a novel device for minimally invasive
percutaneous microresection. Am J Sports Med. 2013 Mar;41(3):636-44.
Liu
WC, Chen CT, Lu CC, Tsai YC, Liu YC, Hsu CW, Shih CL, Chen PC, Fu YC.
Extracorporeal Shock Wave Therapy Shows Superiority Over Injections for
Pain Relief and Grip Strength Recovery in Lateral Epicondylitis: A
Systematic Review and Network Meta-analysis. Arthroscopy. 2022
Jun;38(6):2018-2034.e12.
McShane JM,
Nazarian LN, Harwood MI. Sonographically guided percutaneous needle
tenotomy for treatment of common extensor tendinosis in the elbow. J
Ultrasound Med. 2006 Oct;25(10):1281-9.