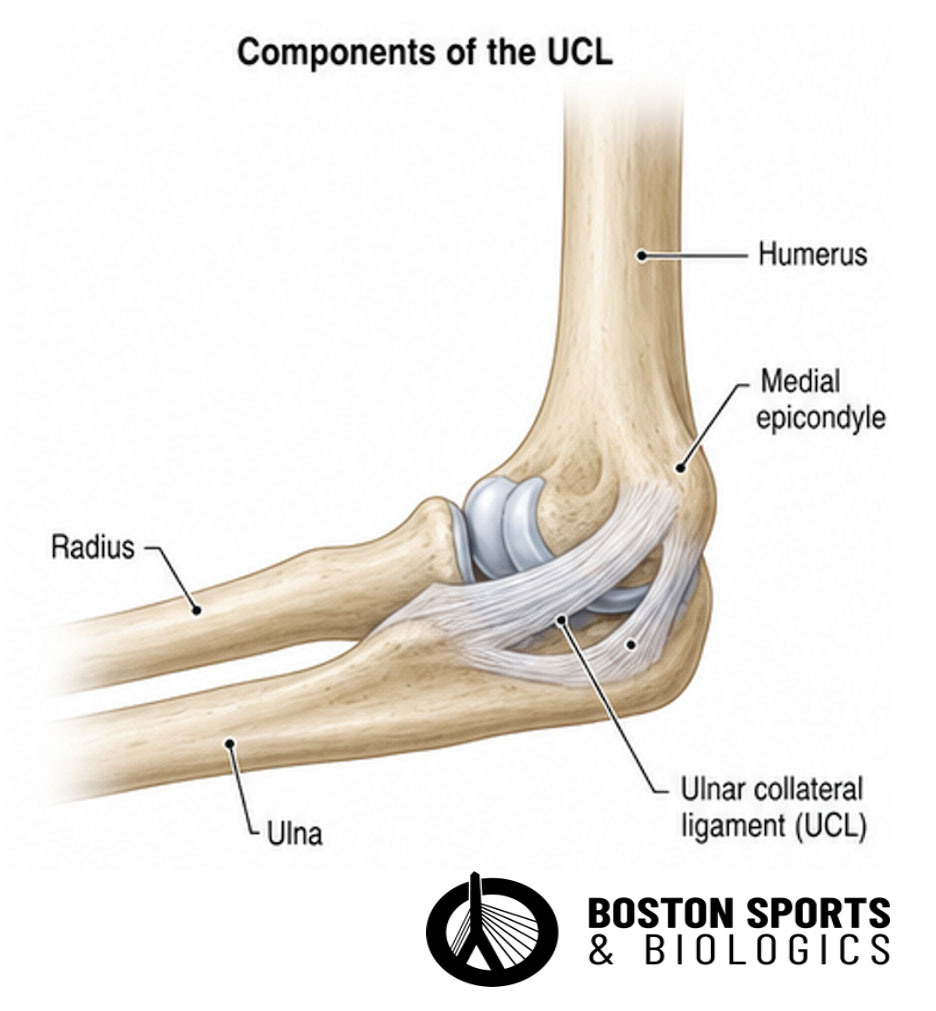
An ulnar collateral ligament (UCL) sprain in the elbow
refers to an injury to the UCL, which is a key stabilizer of the medial
elbow, particularly during activities that involve overhead throwing.
The
UCL is composed of three bundles: anterior, posterior, and transverse,
with the anterior bundle being the primary restraint to valgus stress.
UCL
sprains are common in athletes who participate in overhead sports, such
as baseball pitchers, due to the repetitive valgus stress placed on the
elbow during the throwing motion. This repetitive stress can lead
tomicrotears, partial tears, or complete ruptures of the ligament [Gehrman & Grandizio, 2022; Hariri & Safran, 2010; Carr et al, 2020].
How is a Ulnar Collateral Ligament (UCL) sprain diagnosed?
The diagnosis of an ulnar collateral ligament (UCL) sprain in the elbow involves a combination of clinical evaluation and imaging studies.
History and Physical Examination:
Patients
with a UCL sprain typically present with medial elbow pain, which may
be exacerbated by throwing or other activities that place stress on the
elbow.
Patients may also experience a decrease in throwing velocity and accuracy.
Physical examination findings often include tenderness over the medial
elbow and positive valgus stress tests, such as the moving valgus stress
test and the milking maneuver [Hariri & Safran, 2010; Safran et al, 2005].
Imaging Studies: The diagnosis of a UCL sprain is primarily clinical, supported by imaging studies.
Magnetic Resonance Imaging (MRI):
MRI is considered the gold standard for diagnosing UCL injuries. It
provides detailed visualization of the ligament, showing signs of
laxity, irregularity, and increased signal intensity, which indicate
injury. MRI has a sensitivity and specificity ranging from 57% to 100%
and 89% to 100%, respectively [Mirowitz & London, 1992; Campbell et al, 2020].
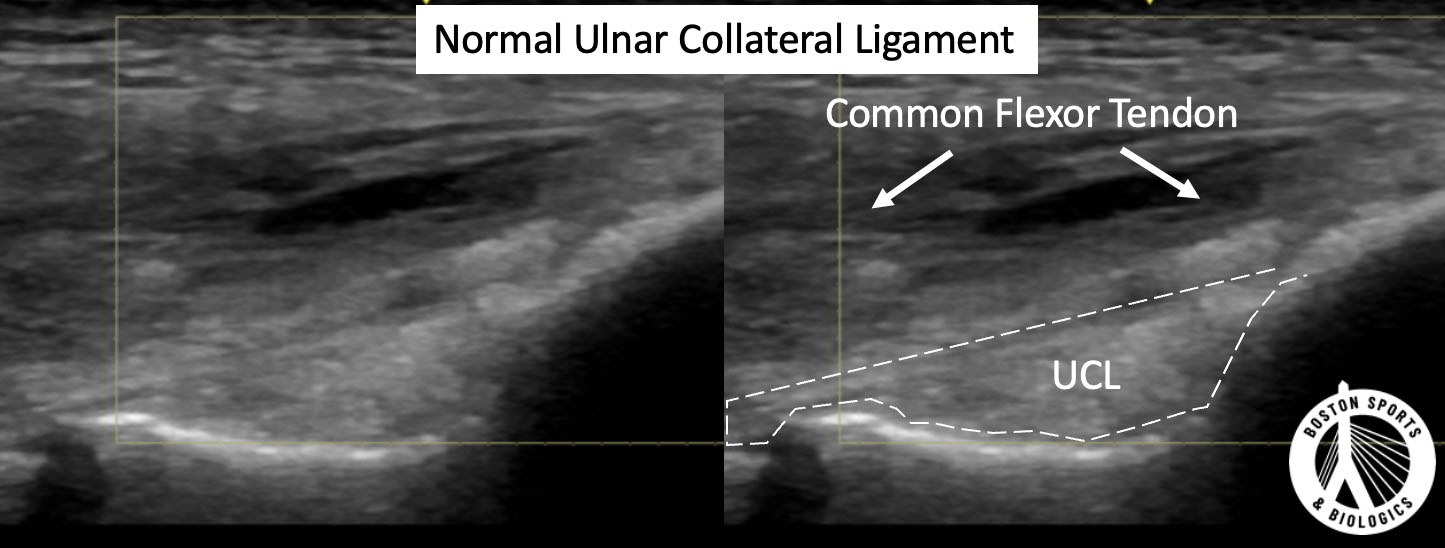
Ultrasound (US):
Conventional and stress ultrasound are valuable, especially for dynamic
assessment. Conventional US has a sensitivity of 79% and specificity of
98% for full-thickness tears, while stress US has a sensitivity of 96%
and specificity of 81%. Stress US can measure joint gapping under valgus
stress, correlating with the severity of UCL injury [Ciccotti & Ciccotti, 2020; Thomas et al, 2022; Park et al, 2020].
What are the treatments for a Ulnar Collateral Ligament (UCL) sprain?
Non-surgical treatment options for an ulnar collateral ligament (UCL) sprain in the elbow include several approaches aimed at reducing pain, promoting healing, and restoring function. These options are particularly effective for low- to medium-grade partial tears (grade I or II).
Rest and Activity Modification: Initial management involves rest from aggravating activities, particularly throwing, to allow the ligament to heal. Activity modification is crucial to prevent further injury [Hariri & Safran, 2010; Carr et al, 2020].
Physical Therapy: A structured rehabilitation program focusing on strengthening the flexor-pronator muscles, improving range of motion, and gradually progressing to sport-specific activities is essential. Physical therapy alone has shown a return to sport (RTS) rate of approximately 79.7% [Gopinatth et al, 2023].
Bracing: The use of a hinged elbow brace can provide support and limit valgus stress on the elbow during the healing process, particularly in younger athletes [Savoie & O'Brien, 2020].
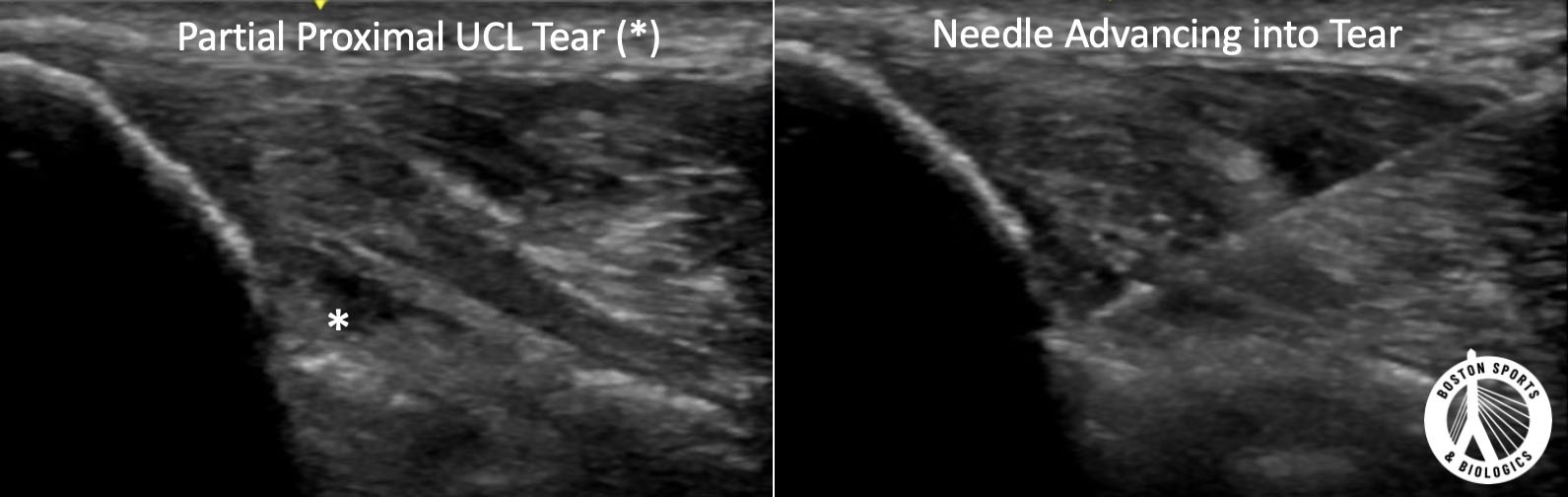
Platelet-Rich Plasma (PRP) Injections: PRP injections
have been used to promote healing of partial UCL tears.
A case series by Podesta et al. evaluated 34 athletes with partial UCL tears who received a single type 1A PRP injection under ultrasound guidance. At an average follow-up of 70 weeks, 88% of athletes returned to the same level of play without complaints. Significant improvements were noted in the Kerlan-Jobe Orthopaedic Clinic (KJOC) score (from 46 to 93) and the Disabilities of the Arm, Shoulder, and Hand (DASH) score (from 21 to 1) [Podesta et al, 2013].
A systematic review by Fucaloro et al. analyzed eight studies involving 278 partial-thickness and 44 full-thickness UCL tears. The return to sport (RTS) rates ranged from 46% to 100%, with higher success rates observed in studies with longer rehabilitation programs (12-14 weeks) and those using leukocyte-poor PRP. The RTS rates for partial-thickness tears ranged from 59% to 100% [Fucaloro et al, 2024].
Chauhan et al. conducted a comparative study on professional baseball players, showing that PRP did not significantly improve return to play (RTP) outcomes compared to non-PRP treatment. However, variability in PRP preparations and rehabilitation protocols may have influenced these results [Chauhan et al, 2019].
A systematic review and meta-analysis by Gopinatth et al. found no significant difference in RTS rates between athletes treated with PRP and those who did not receive PRP. The overall RTS rate for nonoperative management, including PRP, was 79.7% [Gopinatth et al, 2023].
Surgical
Surgical approaches for ulnar collateral ligament (UCL) sprains in the elbow primarily include UCL reconstruction (UCLR) and UCL repair with suture augmentation.
UCL Repair with Suture Augmentation: This approach is typically used for acute injuries, minimal ligamentous
degeneration, or isolated proximal or distal avulsions [Pezzulo et al, 2024; Dugas et al, 2025; Spears et al, 2024] and RTP rates ranging from 92% to 96% and a shorter time to return to play (approximately 6 months) compared to UCLR [Dugas et al, 2025; Spears et al, 2024].
What is the average recovery time post-surgery for UCL sprains?
The average recovery time post-surgery for ulnar collateral ligament (UCL) sprains in the elbow varies depending on the surgical approach used.
For UCL reconstruction (UCLR): The Modified Jobe Technique has an average time to return to full competition is 12 to 15 months, with professional pitchers often requiring 15 to 18 months to return to their previous level of competition [Carr et al, 2020]. TheDocking Technique typically results in a return to play (RTP) at around 12 to 18 months post-surgery, with a high success rate of approximately 90% [Pezzulo et al, 2024].
For UCL repair with suture augmentation: This approach has shown a shorter recovery time, with athletes generally returning to sport in approximately 6 to 9 months. The RTP rate is high, ranging from 92% to 96% [Dugas et al, 2025; Spears et al, 2024].
What are the potential complications following UCL surgery in the elbow?
Common complications following ulnar collateral ligament (UCL) surgery in the elbow, considering both UCL reconstruction and UCL repair with suture augmentation, include:
Ulnar Neuropathy: This is the most frequently reported complication. The incidence of postoperative ulnar neuropathy varies, with rates reported as high as 12% overall for UCL reconstruction. Ulnar nerve transposition, particularly submuscular transposition, is associated with higher rates of ulnar neuropathy [Looney et al, 2021; Clain et al, 2019].
Revision Surgery: UCL repair with suture augmentation has been associated with a higher risk of revision surgery compared to UCL reconstruction. The estimated 2-year revision-free survival was 99.5% for UCL reconstruction compared to 97.9% for UCL repair [Varady et al, 2024].
Persistent Ulnar Nerve Symptoms: Persistent ulnar nerve symptoms post-surgery are reported in a small percentage of patients, particularly those who underwent concomitant ulnar nerve transposition [Hones et al, 2024].
Infection and Wound Complications: Although less common, infection and wound complications can occur postoperatively. These are generally managed with appropriate medical or surgical interventions.
Graft Failure: Graft failure, although rare, can occur and may necessitate revision surgery. The choice of graft (autograft vs. allograft) can influence the risk of graft failure, with allografts associated with a higher revision rate [Hones et al, 2024].
Other Nerve-Related Complications: Other nerve-related complications, such as transient paresthesia, can occur, particularly in athletes involved in high-stress activities like gymnastics and javelin throwing [Jones et al, 2014].
A UCL tear is an injury to the ulnar collateral ligament, the primary stabilizing ligament on the inside of the elbow. UCL tears are common in baseball pitchers, quarterbacks, javelin throwers, and other overhead athletes. The injury can range from a mild sprain to a complete ligament rupture.
A UCL sprain refers to stretching or minor damage to the ligament. A
partial UCL tear involves disruption of some ligament fibers, while a
complete UCL tear means the ligament has ruptured entirely. Treatment
options vary based on the severity and location of the injury.
Yes. Many athletes with partial UCL tears successfully return to
sports without surgery. Non-surgical treatment may include physical
therapy, throwing rehabilitation programs, platelet-rich plasma (PRP)
injections, and other biologic treatments.
No. Many UCL injuries do not require Tommy John surgery. Athletes
with partial tears, lower-demand athletes, and recreational athletes can
often recover with nonoperative treatment. Surgery is generally
reserved for complete tears or athletes who fail conservative care.
Tommy John surgery, also known as UCL reconstruction, involves
replacing the injured ligament with a tendon graft. The procedure is
commonly performed in competitive throwing athletes who have complete
tears or significant elbow instability.
PRP and Tommy John surgery treat different degrees of injury. PRP is
often considered for partial tears and chronic ligament degeneration,
while Tommy John surgery is typically reserved for complete tears or
athletes who do not improve with conservative treatment.
Campbell RE, McGhee AN, Freedman KB, Tjoumakaris FP. Diagnostic Imaging of Ulnar Collateral Ligament Injury: A Systematic Review. Am J Sports Med. 2020 Sep;48(11):2819-2827.
Chauhan A, McQueen P, Chalmers PN, Ciccotti MG, Camp CL, D'Angelo J, Potter HG, Fealy SA, Erickson BJ, Hoenecke HR, Keefe D, McCauley J, Fronek J. Nonoperative Treatment of Elbow Ulnar Collateral Ligament Injuries With and Without Platelet-Rich Plasma in Professional Baseball Players: A Comparative and Matched Cohort Analysis. Am J Sports Med. 2019 Nov;47(13):3107-3119.
Clain JB, Vitale MA, Ahmad CS, Ruchelsman DE. Ulnar Nerve Complications After Ulnar Collateral Ligament Reconstruction of the Elbow: A Systematic Review. Am J Sports Med. 2019 Apr;47(5):1263-1269.
Dugas JR, Froom RJ, Mussell EA, Carlson SM, Crawford AE, Tulowitzky GE, Dias T, Wilk KE, Patel AN, Kidwell-Chandler AL, Ryan MK, Atkinson AW, Manush AH, Rothermich MA, Ithurburn MP, Emblom BA, Cain EL Jr. Clinical Outcomes of Ulnar Collateral Ligament Repair With Internal Brace Versus Ulnar Collateral Ligament Reconstruction in Competitive Athletes. Am J Sports Med. 2025 Jan 31:3635465251314054.
Fucaloro SP, Kang AS, Bragg JT, Krivicich L, Salzler MJ. Return to Sport After Ulnar Collateral Ligament Tears Treated with Platelet-Rich Plasma Injections is Influenced by Length of Rehabilitation and Leukocyte Content of Injections: A Systematic Review. Arthroscopy. 2025 Feb;41(2):343-356.
Gehrman MD, Grandizio LC. Elbow Ulnar Collateral Ligament Injuries in Throwing Athletes: Diagnosis and Management. J Hand Surg Am. 2022 Mar;47(3):266-273.
Gopinatth V, Batra AK, Khan ZA, Jackson GR, Jawanda HS, Mameri ES, McCormick JR, Knapik DM, Chahla J, Verma NN. Return to Sport After Nonoperative Management of Elbow Ulnar Collateral Ligament Injuries: A Systematic Review and Meta-analysis. Am J Sports Med. 2023 Dec;51(14):3858-3869.
Hariri S, Safran MR. Ulnar collateral ligament injury in the overhead athlete. Clin Sports Med. 2010 Oct;29(4):619-44.
Hones KM, Simcox T, Hao KA, Portnoff B, Buchanan TR, Kamarajugadda S, Kim J, Wright JO, King JJ, Wright TW, Schoch BS, Aibinder WR. Graft choice and techniques used in elbow ulnar collateral ligament reconstruction over the last 20 years: a systematic review and meta-analysis. J Shoulder Elbow Surg. 2024 May;33(5):1185-1199.
Jones KJ, Dines JS, Rebolledo BJ, Weeks KD, Williams RJ, Dines DM, Altchek DW. Operative management of ulnar collateral ligament insufficiency in adolescent athletes. Am J Sports Med. 2014 Jan;42(1):117-21.
Looney AM, Wang DX, Conroy CM, Israel JE, Bodendorfer BM, Fryar CM, Pianka MA, Fackler NP, Ciccotti MG, Chang ES. Modified Jobe Versus Docking Technique for Elbow Ulnar Collateral Ligament Reconstruction: A Systematic Review and Meta-analysis of Clinical Outcomes. Am J Sports Med. 2021 Jan;49(1):236-248.
Mirowitz SA, London SL. Ulnar collateral ligament injury in baseball pitchers: MR imaging evaluation. Radiology. 1992 Nov;185(2):573-6.
Park JY, Kim H, Lee JH, Heo T, Park H, Chung SW, Oh KS. Valgus stress ultrasound for medial ulnar collateral ligament injuries in athletes: is ultrasound alone enough for diagnosis? J Shoulder Elbow Surg. 2020 Mar;29(3):578-586.
Pezzulo J, Johns WL, Erickson BJ, Ciccotti MG, Ciccotti MC. Evolution of the Surgical Treatment of Ulnar CollateralLigament Injuries. Arthroscopy. 2024 Dec;40(12):2780-2782.
Podesta L, Crow SA, Volkmer D, Bert T, Yocum LA. Treatment of partial ulnar collateral ligament tears in the elbow with platelet-rich plasma. Am J Sports Med. 2013 Jul;41(7):1689-94.
Safran M, Ahmad CS, Elattrache NS. Ulnar collateral ligament of the elbow. Arthroscopy. 2005 Nov;21(11):1381-95.
Savoie FH 3rd, O'Brien M. Sprains, Strains, and Partial Tears of the Medial Ulnar Collateral Ligament of the Elbow. Clin Sports Med. 2020 Jul;39(3):565-574.
Spears TM, Parikh B, Chalmers PN, Smith MV, Freehill MT, Bowman EN. Elbow Ulnar Collateral Ligament Repair With Suture Augmentation Is Biomechanically Equivalent to Reconstruction and Clinically Demonstrates Excellent Outcomes: A Systematic Review. Arthroscopy. 2024 Apr;40(4):1343-1355.e1.
Thomas JM, Chang EY, Ha AS, Bartolotta RJ, Bucknor MD, Caracciolo JT, Chen KC, Flug J, Kumaravel M, Raizman NM, Ross AB, Silvis ML, Surasi DS, Beaman FD. ACR Appropriateness Criteria® Chronic Elbow Pain. J Am Coll Radiol. 2022 Nov;19(11S):S256-S265.
Watson JN, McQueen P, Hutchinson MR. A systematic review of ulnar collateral ligament reconstruction techniques. Am J Sports Med. 2014 Oct;42(10):2510-6.
Varady NH, Parise S, Kunze KN, Brusalis CM, Williams RJ 3rd, Altchek DW, Dines JS. Favorable Outcomes Following Elbow Ulnar Collateral Ligament Reconstruction and Repair, Though Repair Associated with Increased Risk of Revision Surgery. Arthroscopy. 2024 Nov 10:S0749-8063(24)00903-4.
Vitale MA, Ahmad CS. The outcome of elbow ulnar collateral ligament reconstruction in overhead athletes: a systematic review. Am J Sports Med. 2008 Jun;36(6):1193-205.